Quick summary
West Nile virus in the USA tends to peak from late summer into early fall, and the pattern repeats most years. Most infections are mild or silent, but older adults and people with weaker immunity face a higher chance of severe illness. This guide pulls together what Americans need now: a 2025 season overview, links to official state maps, plain-English symptoms and testing, plus a 10-minute yard checklist that actually reduces bites. If you only do three things this week—dump standing water, fix window/door screens, and use an EPA-registered repellent at dusk and dawn—you’ll meaningfully lower your family’s risk.
It is the leading mosquito-borne illness in the U.S., with activity that rises as summer turns into fall. Most people who get infected never feel sick. A smaller group develops a flu-like fever, and a small fraction—especially older adults or those with weakened immunity—can develop serious neurologic complications. The good news: simple weekly habits at home, plus smart protection when you’re outdoors at dusk or dawn, can meaningfully lower your risk.
What to do this week (10 minutes, tops):
- Dump & drain: Empty standing water from buckets, planters, birdbaths, kiddie pools, tarps, gutters, and tires. Refresh birdbaths every 2–3 days.
- Defend your home: Repair or replace torn window and door screens; keep doors closed in the evening.
- Protect yourself: Use an EPA-registered insect repellent (DEET, picaridin, oil of lemon eucalyptus, or IR3535), wear long sleeves and pants at dusk/dawn, and consider light-colored clothing that makes mosquitoes easier to spot.
- Plan your evenings: If you’re hosting sports, cookouts, or outdoor events, add fans, choose well-lit areas with fewer shrubs, and keep a repellent station by the door.
If you or a family member develops severe headache, stiff neck, confusion, weakness, or high fever, seek medical care promptly. Early evaluation helps clinicians decide on testing and supportive treatment.
What is West Nile virus?
West Nile virus is a mosquito-borne virus that cycles primarily between birds and Culex mosquitoes. Humans and other mammals (like horses) are considered “dead-end hosts,” which means the virus doesn’t usually spread onward from us. In practical terms: you don’t catch WNV from touching or talking to someone who is ill, and it isn’t spread through food or drinking water. The usual route is simple—an infected mosquito bites.
For most people, infection is silent: no symptoms at all. Others experience a short-lived illness that looks a lot like a summer virus—fever, headache, body aches, maybe a rash. A small share of infections can become neuroinvasive disease (such as meningitis or encephalitis), which is why public-health guidance focuses so much on prevention for higher-risk groups: adults over 60, people with certain chronic conditions or weakened immune systems, and anyone with frequent evening outdoor exposure during peak mosquito season.
A few features make WNV different from headline-grabbing tropical diseases:
- U.S. seasonality: Risk isn’t year-round. Across much of the country, activity builds in late spring and peaks in late summer through early fall, then tapers as temperatures drop.
- Local patterns matter: Warm weather + recent rain + containers that hold water = more mosquito breeding. Even one neglected bucket or clogged gutter can produce hundreds of mosquitoes.
- Prevention is practical: You don’t need specialized equipment. Screens, weekly yard checks, and a good repellent routine go a long way at the community and household level.
Think of WNV prevention as layers: remove mosquito habitats in your yard, block their entry to your home, protect your skin when mosquitoes are most active, and stay tuned to local health updates during peak months. Those layers work together—and they’re easy to repeat each week until the first cold snap arrives.
When does West Nile season peak?
If you had to circle one window on the calendar, it would be late summer into early fall. That’s when West Nile virus activity typically crests across the United States. The exact timing shifts with temperature, recent rain, and standing water, which is where Culex mosquitoes breed.
How the curve usually looks—region by region
- South & Gulf Coast: The season starts early and runs long; activity often swells July–September.
- Southwest & Desert states: Heat plus monsoon bursts create short, intense waves; peaks land July–August.
- Midwest & Great Plains: Warm, stormy summers drive activity; look for peaks August–September.
- Northeast & Mid-Atlantic: Warmer, wetter summers have nudged risk later; peaks commonly August–September.
- West Coast: Coastal areas may peak later and softer; inland valleys often hit August–October.
Why timing changes from place to place
- Warm evenings: Mosquitoes breed faster and bite more when nights don’t cool off.
- Rain + containers: Buckets, clogged gutters, tires, tarps, and planters can turn into nurseries in just a few days.
- Urban heat islands: Warmer neighborhoods can keep mosquitoes active well into fall.
- Irrigation & water features: Over-watered lawns, rain barrels, and ornamental ponds add reliable breeding spots.
A practical month-by-month guide
- May–June: Get ahead of it—fix window/door screens, set a weekly “dump & drain” routine, stock repellent.
- July: After storms, expect busier evenings; refresh birdbaths every 2–3 days and clear yard clutter.
- August–September (peak): Double down—repellent at dusk/dawn, long sleeves, fans on patios, and no standing water.
- October: Keep the routine going until nights stay cool; fall clean-ups (gutters, tarps, planters) pay off.
Signals your local risk is rising
- New posts from your county health department or vector control
- Reports of positive mosquito pools or dead-bird testing
- A noticeable jump in evening mosquitoes after a warm, rainy stretch
Bottom line: plan on a late-summer peak every year and keep simple yard and personal-protection habits running until the first reliable cool snap.
How WNV spreads (and how it doesn’t)
Picture the cycle like a loop in nature. Birds carry West Nile virus in the wild. A Culex mosquito bites an infected bird and picks up the virus. After a short incubation inside the mosquito, that same mosquito can pass the virus along the next time it feeds—on another bird, or on a human or horse. Humans and horses are considered dead-end hosts: the virus doesn’t reach levels in our blood high enough to keep the chain going.
What happens after a bite
If illness develops, symptoms usually appear 2–14 days later (sometimes a bit longer in people with weakened immunity). Most infections are silent. Some feel like a brief summer virus—fever, headache, body aches, maybe a rash. A small fraction progress to neuroinvasive disease (meningitis or encephalitis), which needs urgent medical care.
Routes that exist, but are uncommon
- Blood transfusion or organ transplant from an infected donor (screening has made this rare).
- Laboratory exposure in specialized settings.
- Pregnancy/breastfeeding: documented infrequently; clinicians assess risks individually.
Ways you won’t catch West Nile
- Not person-to-person through casual contact, coughing, or sharing food.
- Not from touching someone who’s sick with WNV.
- Not via properly treated water (like chlorinated pools) or cooked foods.
- Not from pets through everyday contact—pets are at risk from mosquito bites, just like us.
Why evenings matter so much
Culex mosquitoes are most active at dusk and dawn. That’s the window when repellent, long sleeves, and even a box fan on the porch make the biggest difference.
Takeaway: break the chain at the easy points—eliminate standing water, keep screens tight, and protect exposed skin during prime mosquito hours.
Who’s most at risk?
West Nile virus can affect anyone, but the chance of severe illness isn’t the same for everyone. These factors raise risk and deserve extra attention during peak season:
Health & age factors
- Older adults (≈60+) — higher likelihood of neuroinvasive disease (meningitis, encephalitis) and hospitalization.
- Weakened immunity — transplant recipients, people on chemotherapy or high-dose steroids, those with advanced HIV, or other conditions that blunt immune response.
- Chronic conditions — diabetes, kidney disease, cancer, or uncontrolled hypertension can complicate recovery.
Exposure factors
- Evening outdoor time — Culex mosquitoes prefer dusk and dawn. Regular gardening, dog-walking, outdoor sports, or porch sitting at these hours increases bite risk.
- Standing water near home — planters, gutters, birdbaths, kiddie pools, tires, tarps, rain barrels, and poorly drained yards create breeding sites.
- Limited window/door screening — torn screens or frequently propped-open doors make indoor bites more likely.
- Outdoor occupations — construction, landscaping, utilities, farming, park services, and event staff spend long stretches outside.
- Communities with less vector control — fewer larvicide programs, infrequent storm-drain maintenance, or rare adult-mosquito spraying mean more bites reach people.
Pregnancy & children
Pregnant people and infants should follow the same prevention layers as everyone else: remove standing water, use EPA-registered repellent as directed, and rely on screens and protective clothing at dusk/dawn. If you’re pregnant and develop fever with severe headache, neck stiffness, confusion, or weakness, seek care promptly.
Practical ways to lower personal risk
- Make repellent a habit before evening activities.
- Keep long sleeves/pants by the door for dusk/dawn.
- Run a box fan on porches/patios—moving air makes it harder for mosquitoes to land.
- Set a weekly “dump & drain” reminder on your phone until nights turn cool.
Symptoms & when to get medical care
Most people infected with West Nile virus never feel sick. Among those who do, illness ranges from a short, flu-like fever to rare but serious neurologic disease. Knowing what to watch for helps you decide when to rest at home—and when to call a clinician.
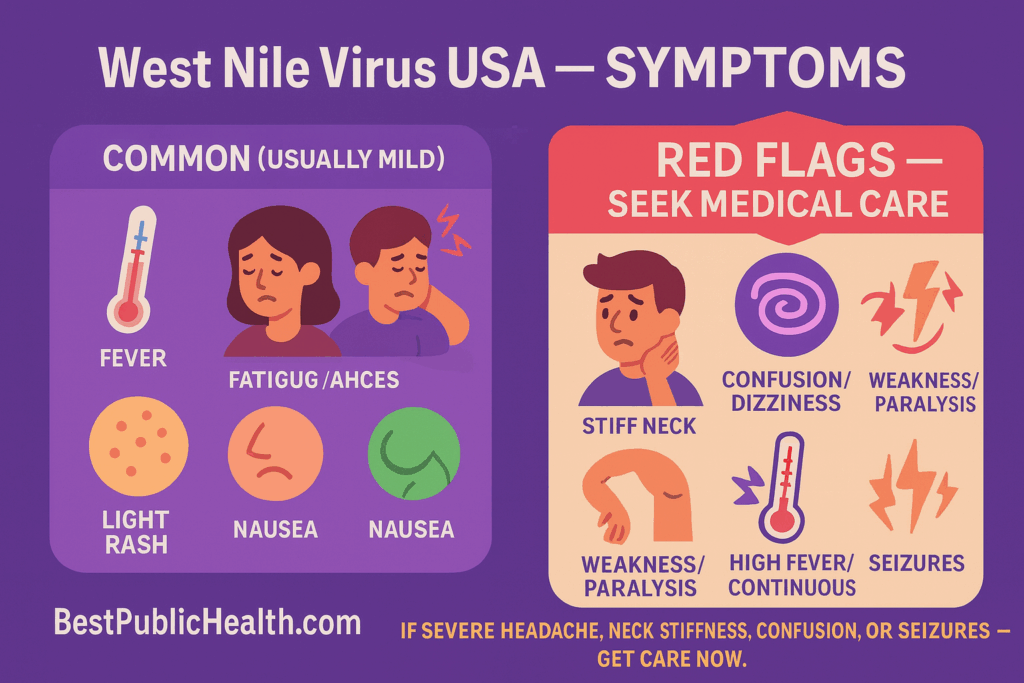
Common, usually mild (“West Nile fever”)
- Fever, headache, fatigue
- Body aches or joint pains
- Occasional rash (more often on the trunk)
- Nausea or mild stomach upset
These symptoms typically start 2–14 days after a bite and resolve over several days to a couple of weeks. Fatigue can linger a bit longer for some people.
Serious, less common (neuroinvasive disease) — needs urgent care
- Severe headache or high fever that doesn’t improve
- Neck stiffness, sensitivity to light
- Confusion, disorientation, personality changes
- Weakness in an arm or leg, trouble walking, new drooping on the face
- Tremors, seizures, or loss of consciousness
If any of the red-flag symptoms appear—especially in older adults or people with weakened immune systems—seek medical care immediately (ER or urgent care). Clinicians decide on testing based on symptoms and timing; there’s no specific antiviral for West Nile virus, so treatment focuses on supportive care (fluids, fever control, monitoring, and hospital care if needed).
At-home care for mild illness
- Rest and hydrate. Small, frequent sips if nausea is present.
- Fever and pain relief with standard over-the-counter options if your clinician says they’re safe for you.
- Avoid strenuous activity until you’re clearly improving.
Call a clinician promptly if:
- Fever lasts more than 3 days, or symptoms worsen instead of improving.
- You have a chronic condition, are pregnant, or care for an older adult who develops concerning symptoms.
- New neurologic signs appear at any point (weakness, confusion, severe headache, seizures).
This guide is educational and not a diagnosis. If you’re worried about your symptoms, err on the side of calling your healthcare provider or seeking urgent care—especially during West Nile season.
West Nile testing, diagnosis & treatment: when it’s worth a test
Doctors don’t test everyone with a summertime fever. West Nile testing is usually considered when the timing and symptoms line up—you’re in mosquito season and have red-flag signs such as a severe headache, stiff neck, confusion, new weakness, or seizures, or you’re at higher risk (older age or a weakened immune system). If a mild illness is already improving, a test rarely changes care. If symptoms worsen or linger, that’s the moment to call your clinician and ask whether West Nile testing makes sense.
How testing works (plain English)
- Blood tests for antibodies (IgM): The most common test looks for IgM antibodies your immune system makes soon after infection. These typically show up a few days after symptoms start and can hang around for weeks to months.
- Spinal fluid (CSF) in severe cases: If doctors suspect meningitis or encephalitis, they may analyze spinal fluid and send IgM testing on that sample as well.
- Confirmatory testing: In some situations—like unusual presentations or early/late timing—clinicians may request confirmatory tests from reference labs.
- Viral detection (NAAT/PCR): Less common and most helpful very early in illness; a negative result doesn’t rule out infection.
What results mean
- A positive IgM with the right timing and symptoms supports a recent West Nile infection.
- Equivocal or negative results early on may simply be too soon; clinicians can repeat testing after a short interval if suspicion remains high.
Treatment basics
There’s no specific antiviral for West Nile virus. Care focuses on:
- Fluids, rest, and fever control for mild illness (use only medications that are safe for you; when in doubt, ask your clinician).
- Hospital care for severe disease to manage pain, hydration, breathing, seizures, or neurologic complications.
- Rehabilitation (physical/occupational therapy) if weakness or balance issues persist.
Recovery & follow-up
- Most people with mild illness recover within days to a couple of weeks, though fatigue can linger.
- After severe disease, improvement may be gradual; follow-up with your primary care clinician or neurologist helps track recovery and address lingering symptoms (sleep, mood, strength, balance).
- If new or worsening neurologic signs appear at any time, seek urgent care.
This section is informational and not a substitute for medical advice. If you’re concerned about symptoms—especially during mosquito season—contact a healthcare professional promptly.
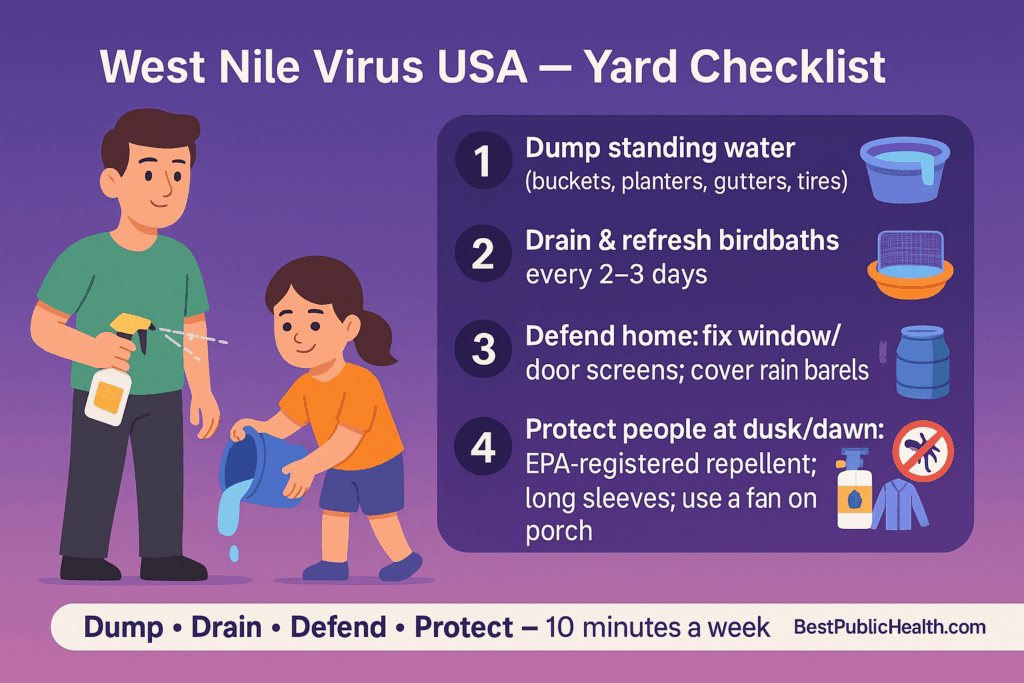
Prevention at home: the 10-minute yard checklist
Mosquito control at home is won in small, repeatable routines. Set a weekly phone reminder and walk your space—front porch, backyard, side yard, balcony.
Your 10-minute routine
- Dump & drain
- Empty buckets, saucers, planters, tarps, toys, tires, and kiddie pools.
- Birdbaths: refresh every 2–3 days.
- Clear clogged gutters and downspouts after storms.
- Seal & screen
- Fix torn window/door screens; ensure doors close fully.
- Cover rain barrels with tight-fitting lids or fine mesh.
- Thin & tidy
- Trim dense shrubs near patios where mosquitoes rest.
- Remove leaf piles and yard clutter that trap water.
- Treat standing water you must keep
- Ornamental ponds or rain barrels: aerate, add fish where appropriate, or use Bti “mosquito dunks” strictly as labeled.
- Never pour oil, bleach, or pesticides into natural water or storm drains.
- Protect people (especially at dusk/dawn)
- Keep a repellent basket by the door.
- Add a box fan to porches/patios—moving air makes landings harder.
- Wear long sleeves/pants for evening yard time; choose light colors to spot mosquitoes better.
Quick guide to EPA-registered repellents (check each product’s label for age limits, % concentration, and reapply times)
| Active ingredient | Typical everyday use | Notes |
|---|---|---|
| DEET (20–30%) | Reliable protection for several hours | Widely studied; use lowest effective % for your outing |
| Picaridin (20%) | Long-lasting, low-odor option | Good on skin and clothing; non-greasy feel |
| Oil of Lemon Eucalyptus (OLE/PMD) (~30%) | Plant-derived, several hours’ protection | Not for children under 3; follow label closely |
| IR3535 | Moderate-to-long protection | Common in multi-use products; check specific reapply guidance |
Pro tips that make a big difference
- After every rain, do a fast sweep of the yard—water can collect and hatch mosquitoes in just a few days.
- Store items upside-down (buckets, wheelbarrows) so they can’t collect water.
- Share the checklist with neighbors; mosquitoes don’t respect fences.
- For community living (HOAs, apartments), ask about storm-drain maintenance and scheduled larvicide programs.
Set it and forget it (almost): Make the routine weekly from May–October (or until nights are reliably cool). Those minutes pay back with quieter evenings, fewer bites, and lower risk all season.
Community & school prevention
Mosquito control works best when neighbors, schools, and parks pull in the same direction. A few coordinated tweaks can shrink breeding sites across an entire block.
Neighborhood actions that move the needle
- Storm drains & gutters: Ask public works or your HOA about clearing leaves and sediment after big rains. Clogged drains are mosquito factories.
- Vacant lots & “green pools”: Report neglected swimming pools, water-filled construction pits, and trash piles to your vector control district.
- Tire & junk clean-ups: Old tires trap water for months. Organize a tire amnesty day or bulk-trash pickup after storms.
- Rain-smart landscaping: Add gravel under downspouts, level tarp low spots, and choose planters with drainage.
- Get on the list: Sign up for your county’s mosquito spraying and larvicide notifications so residents know when and why treatments happen.
Schools, camps, and child-care
- Practice schedules: Nudge outdoor practices away from dusk and dawn when Culex are most active.
- Facilities: Keep window/door screens intact; fix gaps on portables and gym side doors.
- Play yards: Empty water from toys, sand-toy bins, and tarps after every rain.
- Shade + fans: Box fans at entries and covered areas make it harder for mosquitoes to land.
- Repellent policy: Share a short, plain-English note for parents on EPA-registered repellents and how the school handles field days or evening events.
Copy-paste bulletin for your newsletter/parent email
“Mosquito season peaks in late summer. Please help us keep the campus bite-free: send students in light long sleeves for evening events, consider an EPA-registered repellent, and dump standing water after rain (buckets, toys, tarps). We monitor storm drains and refresh play-area water regularly. Questions? Contact [School Health Office] or visit [County Vector Control].”
Outdoor work, sports & travel tips
Whether you’re coaching under the lights, running a jobsite, or road-tripping across states, a few habits cut risk without slowing you down.
For outdoor workers & employers
- Repellent kit on site: Stock EPA-registered repellent where crews clock in; remind workers to reapply per the label, especially for dusk tasks.
- Break areas that block bites: Shade, fans, and intact screens on trailers or tents.
- Uniform hacks: Light-colored long sleeves/pants; consider permethrin-treated clothing (follow product directions).
- Post-rain walk-throughs: Drain tarps, wheelbarrows, equipment buckets, and scaffold bases that hold water.
- Toolbox talk: Add a 60-second West Nile reminder to weekly safety meetings during peak months.
For coaches, leagues, and evening rec
- Game-time shifts: When possible, avoid start times at dusk. If not, boost fans at benches and sideline tents.
- Team checklist: Repellent pump by the gear bin, extra long-sleeve warm-ups, and a quick tarp sweep after rain.
- Field maintenance: Clear clogged drains near bleachers; empty water from cones and training gear.
Events, weddings, and back-yard parties
- Prep the venue: A week out, dump & drain; day-of, run box fans in seating and buffet areas.
- Lighting & layout: Keep guests out of dense shrubs; choose brighter, open spaces where breezes help.
- Courtesy station: Set out repellent wipes/spray with a clear label.
Camping, hiking, and lake weekends
- Screens + zips: Use a tent with tight mesh; keep doors zipped at dusk/dawn.
- Clothing & treatment: Long sleeves/pants; consider permethrin-treated gear (treat in advance per directions).
- Pick dry campsites: Avoid pitches next to slow, stagnant water; after storms, check for new puddles around camp.
U.S. travel planning
- Check before you go: Look up the state West Nile map or surveillance page for your destination.
- Pack smart: Travel-size repellent, light long sleeves, and a small clip-on fan for porches or cabins.
- Lodging: Favor places with AC or well-fitting window screens; keep doors closed in the evening.
Simple rule of thumb: If the sun is low and the air is still, act like it’s “mosquito prime time”—repellent on, sleeves down, and a fan nearby.
Pets & horses: what owners should know
Mosquitoes don’t just bother people—dogs, cats, and horses can be bitten too. Here’s the practical version for animal lovers and barn owners.
Dogs & cats (household pets)
- Risk profile: Pets can be exposed to West Nile virus, but serious illness in dogs and cats appears uncommon. The bigger issue is simple comfort and bite prevention.
- Everyday protection: Keep pets indoors at dusk and dawn, use tight screens, and run a fan where they rest outside—moving air makes landing harder for mosquitoes.
- Repellents: Never apply human repellents (DEET, OLE/PMD, etc.) to pets unless a veterinarian says it’s safe. Ask your vet about pet-safe products or treated collars when appropriate.
- Water & yard care: Change outdoor water bowls daily, dump standing water in planters and toys, and keep grass and shrubs near pet areas trimmed.
Horses (high priority)
- Why they’re different: Horses are more susceptible to severe West Nile disease. The good news—equine vaccines exist. Talk to your veterinarian about primary series + annual boosters, and earlier vaccination in regions with long seasons.
- Barn and paddock habits:
- Fix or add screens to stalls and tack rooms.
- Use fans over stalls during evening hours.
- Drain or fill low spots where water collects after rain.
- Scrub troughs at least twice a week; don’t add anything to drinking water without your vet’s approval.
- Clear gutters, flip unused buckets, and store equipment upside-down so it can’t capture rain.
- Know the warning signs: If a horse shows fever, stumbling, hind-limb weakness, tremors, or behavior changes, call your veterinarian immediately.
Bottom line for animal owners: Reduce bites where your animals live, vaccinate horses, and loop your veterinarian into any prevention plans or symptoms you notice.
2025 map & surveillance: U.S. overview + how to find your state’s updates
When you see a “West Nile map,” you’re usually looking at data compiled from state and local health departments. Human cases, positive mosquito pools, and sometimes infected birds are reported up to a national system. Because it takes time to investigate and confirm cases, most maps are updated weekly and can lag behind the news by a bit.
How to read the national picture
- Big-picture trends: National dashboards show where activity is being detected this season (human cases and environmental findings). Use them to spot regional patterns—for example, late-summer build-up across the Plains or coastal spikes after heavy rain.
- Data types: Look for tabs or legends that separate human cases, mosquito pools, and other surveillance. A county shaded for mosquito activity isn’t the same as confirmed human illness.
- Time stamps matter: Always check the “last updated” note and the epi week listed on the map.
Why state pages are essential
States and counties often publish more granular detail—weekly PDFs, interactive county maps, and alerts about adulticiding (spraying) or larviciding. Some also post dead-bird testing results or neighborhood-level mosquito traps.
Quick steps to find reliable local info
- Search: “[Your State] West Nile virus 2025 map” or “[Your County] vector control West Nile”.
- On the state health site, look for a 2025 “Arboviral” or “Mosquito-borne” page—that’s where weekly updates live.
- Subscribe to email or SMS alerts if your state or county offers them.
- Bookmark both: the state health department page and your local vector control district (where available).
Sample resources to look for (by region)
- California: State West Nile surveillance page + county vector-control dashboards (e.g., Los Angeles, Orange, Sacramento).
- Texas: Arboviral surveillance updates from the Department of State Health Services; many cities post local trap results.
- Florida: Weekly mosquito-borne illness reports and county health department advisories.
- Arizona: State summaries plus county vector programs (Maricopa, Pima) with trap maps.
- New York: State updates and, for NYC, a dedicated mosquito surveillance portal.
- Illinois: IDPH county maps and seasonal advisories; Chicago posts separate city updates.
Pro tip for readers: Use the national dashboard to understand where the season is heating up, then rely on your state and county pages for decisions about sports schedules, outdoor events, and neighborhood clean-ups. The combination gives you both the trend and the details that matter where you live.
State mini-guides (fast answers for where you live)
Use these as quick references now, then build out full state pages later. Each blurb targets common searches like “West Nile virus [State] 2025 map” and “West Nile season [State].”
California — West Nile virus, season & where to check
At a glance: Long, dry summers plus irrigation mean activity can stretch July–October, peaking late summer—especially in inland valleys.
Where to check updates: Search “California West Nile 2025 surveillance” and your county vector control (e.g., Los Angeles, Orange, Sacramento). Most counties post trap and spray notices weekly.
Local prevention cues: Clean backyard fountains, refresh birdbaths every 2–3 days, and keep rain barrels tightly covered. Desert and valley yards: watch irrigation overspray that puddles overnight.
When to seek care: Any severe headache, stiff neck, confusion, weakness, or high fever—especially in adults 60+.
Bookmark CTA: Save your county vector-control page + state surveillance page. Check after heat + rain bursts.
Texas — West Nile virus, season & where to check
At a glance: Season can start early and run long in much of Texas. Peaks commonly July–September, with local spikes after storms.
Where to check updates: Search “DSHS arboviral 2025 West Nile Texas” plus your city/county health department (many post mosquito pool results and spray schedules).
Local prevention cues: Drain low spots after big rains, store buckets/wheelbarrows upside-down, and monitor storm drains near the curb.
When to seek care: Worsening fever with severe headache, neck stiffness, confusion, or new weakness → urgent care/ER.
Bookmark CTA: Follow your city alerts for adulticiding/larviciding and subscribe to email/text updates.
Florida — West Nile virus, season & where to check
At a glance: Warm, wet stretches can support activity from late spring through fall; coastal and inland wetlands add persistent breeding sites.
Where to check updates: Search “Florida mosquito-borne illness report West Nile 2025” and your county health department for advisories.
Local prevention cues: Empty planter saucers, kayaks, coolers, and pool covers after storms; trim dense hedges around patios.
When to seek care: Any neurologic symptoms or high fever that doesn’t improve—especially in older adults or those with chronic illness.
Bookmark CTA: Keep the state weekly report and your county page handy during summer evenings.
Arizona — West Nile virus, season & where to check
At a glance: Monsoon rains can trigger short, intense bursts of activity, often peaking July–August in metro areas.
Where to check updates: Search “Arizona West Nile 2025 surveillance” plus your county vector programs (e.g., Maricopa, Pima) for trap maps and pool positives.
Local prevention cues: After storms, walk your yard/balcony: dump plant trays, tarps, and patio furniture cups that collect water.
When to seek care: Severe headache, stiff neck, confusion, or new weakness—don’t wait.
Bookmark CTA: Sign up for county mosquito notifications during monsoon season.
New York — West Nile virus, season & where to check
At a glance: Activity typically peaks August–September. Urban heat islands (NYC/Long Island) can extend evening mosquito activity.
Where to check updates: Search “New York West Nile 2025” and, for NYC, “NYC mosquito surveillance” for trap results and spray alerts.
Local prevention cues: Clear backyard clutter, fix window screens, and keep basement stairwell drains free of debris.
When to seek care: Neuro symptoms or high fever + severe headache warrant prompt evaluation.
Bookmark CTA: Follow city/community board alerts for spray schedules, and keep a repellent kit by the door.
Illinois — West Nile virus, season & where to check
At a glance: Warm, stormy summers fuel activity; peaks often August–September across the state.
Where to check updates: Search “Illinois West Nile 2025 county map” and your county health department for weekly arboviral reports.
Local prevention cues: Clean gutters after downpours, empty kids’ toys and rain-catching tarps, and mow areas near stormwater ditches.
When to seek care: Severe headache, stiff neck, confusion, weakness, or seizures—seek urgent care.
Bookmark CTA: Add state + county pages to your bookmarks bar and check after heat + rain cycles.
Tip for all states: Pair your state dashboard with your county vector-control site. The state gives trend context; the county tells you when and where they’re treating mosquitoes.
Myths vs facts: clearing up common West Nile questions
Myth 1: “Only swamps have West Nile.”
Fact: A single bucket, tire, or clogged gutter can hatch hundreds of mosquitoes. Suburban patios and city alleys create just as much risk as wetlands.
Myth 2: “Bug zappers solve the problem.”
Fact: Zappers rarely target the Culex mosquitoes that spread West Nile. They mainly kill non-biting insects. Source reduction (dumping water) and repellent are far more effective.
Myth 3: “All mosquitoes spread West Nile.”
Fact: Risk concentrates in Culex species. Other mosquitoes bite, but not all are efficient West Nile vectors. Focus your effort on standing-water control and dusk/dawn protection.
Myth 4: “Repellents aren’t safe.”
Fact: EPA-registered repellents (DEET, picaridin, OLE/PMD, IR3535) have safety data and clear label directions. Use the lowest effective concentration for your plans and reapply as directed.
Myth 5: “Natural oils work just as well.”
Fact: Some plant-based products offer shorter protection than EPA-registered options. If you’re out at dusk/dawn, pick an EPA-registered active and carry it with you.
Myth 6: “Once you’ve had West Nile, you’re set for life.”
Fact: Infection can provide some immunity, but protection may not be complete or lifelong. Prevention still matters in future seasons.
Myth 7: “Pools make it worse.”
Fact: Properly chlorinated, maintained pools aren’t the problem. It’s untreated water—covers that puddle, unused kiddie pools, planters, and neglected fountains—that drive breeding.
Myth 8: “Cool nights mean zero risk.”
Fact: Activity drops with cooler temps, but risk doesn’t disappear overnight. Keep habits up until nights are consistently cool and your state reports the season winding down.
Myth 9: “Spraying alone will fix it.”
Fact: Community spraying is one layer. The fastest gains happen when households dump & drain standing water and use repellent during peak hours—every block helps.
Takeaway: Skip the shortcuts. The winning combo is source reduction at home, screens that fit, and EPA-registered repellent when the sun is low.
FAQ
Mosquitoes that spread West Nile (mainly Culex species) are most active at dusk and dawn. Plan protection—repellent, long sleeves, fans, and screens—especially during those hours. (CDC)
Choose an EPA-registered repellent with DEET, picaridin, oil of lemon eucalyptus/PMD, or IR3535 and follow the label. Do not use any repellent on babies under 2 months; use netting and clothing instead. Avoid OLE/PMD on children under 3 years. (CDC)
No licensed human vaccine or specific antiviral treatment exists in the U.S. Prevention—repellent, clothing, and mosquito control—is the best protection. (CDC)
Testing is considered when symptoms fit and occur in mosquito season—especially with neurologic signs (severe headache, stiff neck, confusion, weakness, seizures). Diagnosis is usually by WNV-specific IgM in serum or CSF; IgM often becomes detectable 3–8 days after symptom onset (early tests can be negative and may need repeating). (CDC)
Culex mosquitoes can go from egg to biting adult in ~7–10 days in warm weather. Expect more activity within a week after heat + rain unless standing water is dumped or treated. (CDC)
They’re not effective at reducing biting mosquitoes that spread West Nile. Focus on eliminating standing water and using EPA-registered repellent instead. (SGV Mosquito Control, American Mosquito Control Association)
Yes. Screens and AC help keep mosquitoes out of living spaces and are part of CDC’s core prevention advice. (CDC)
Well-maintained, chlorinated pools with circulating water are not mosquito nurseries; neglected or stagnant pools can be. Keep pools maintained and empty kiddie pools when not in use. (US EPA, CDC, Florida Department of Health)
Most people who recover from West Nile are believed to have long-lasting (often lifelong) immunity; people with weakened immune systems may have a less durable response. Prevention still matters every season. (CDC)
Typically 2–6 days (range 2–14 days); it can be longer in people with weakened immunity. (CDC)
Horses are susceptible, but vaccines for horses are available—talk to a veterinarian about primary series and annual boosters (sometimes more often in high-risk regions). For household pets, routine mosquito-bite prevention is the main focus. (AAEP)
References & resources (authoritative)
- CDC — West Nile: Prevention & Key Messages (repellents, dusk/dawn, screens/AC, larvicides). (CDC)
- CDC — Clinical testing & diagnosis (IgM in serum/CSF; timing). (CDC)
- CDC — Clinical signs & symptoms (incubation period, immunity note). (CDC)
- CDC — Symptoms, diagnosis & treatment (patient page). (CDC)
- CDC — Life cycle of Culex mosquitoes (7–10 days egg to adult). (CDC)
- EPA — Using insect repellents safely & effectively (ingredient guidance, OLE/PMD label notes). (US EPA)
- CDC — Preventing mosquito bites (children’s guidance) (no repellent for <2 months; OLE/PMD not <3 years). (CDC)
- CDC — Mosquito control at home (weekly dump/scrub/cover; containers & pools; rain barrels). (CDC)
- State public health examples — pools & WNV (maintained pools aren’t a WNV water hazard; neglected pools can breed mosquitoes). (westnile.ca.gov, Florida Department of Health)
- AAEP — West Nile vaccination guidelines for horses (primary series + annual boosters; risk-based schedules). (AAEP)
This guide is educational and not a substitute for medical advice. If you or a family member has concerning symptoms—especially neurologic signs—seek medical care promptly.
