
Global Health vs Public Health: Why Students Get Confused
If you’ve been scrolling through US university websites, you’ve probably seen both “Global Health” and “Public Health” degrees and thought:
“These sound the same. What’s the actual difference, and which one should I pick?”
Table of Contents
You’re not imagining it – there’s real overlap. Both fields care about population health, not just individual patients. Both talk about prevention, policy, equity, and systems, and both show up under the same schools or departments in the US (usually “Schools of Public Health”). (ceph.org)
Under the hood, though, they’re not identical:
- Public health is traditionally about protecting and improving the health of people in a particular place – for example, US communities, states, or the entire country. Classic definitions describe it as “the science and art of preventing disease, prolonging life, and promoting health through the organized efforts of society.” (sph.rutgers.edu)
- Global health, as defined by Koplan and colleagues and widely used by US universities, is “an area for study, research, and practice that places a priority on improving health and achieving equity in health for all people worldwide,” emphasizing transnational health issues and equity. (The Lancet)
Put bluntly:
- Public health = “How do we protect and improve health in our own systems and communities (often within the US)?”
- Global health = “How do we tackle health problems and inequities that cut across borders and power structures?”
For you as a prospective student in or targeting the US, this isn’t just a semantic debate. The label on your degree influences:
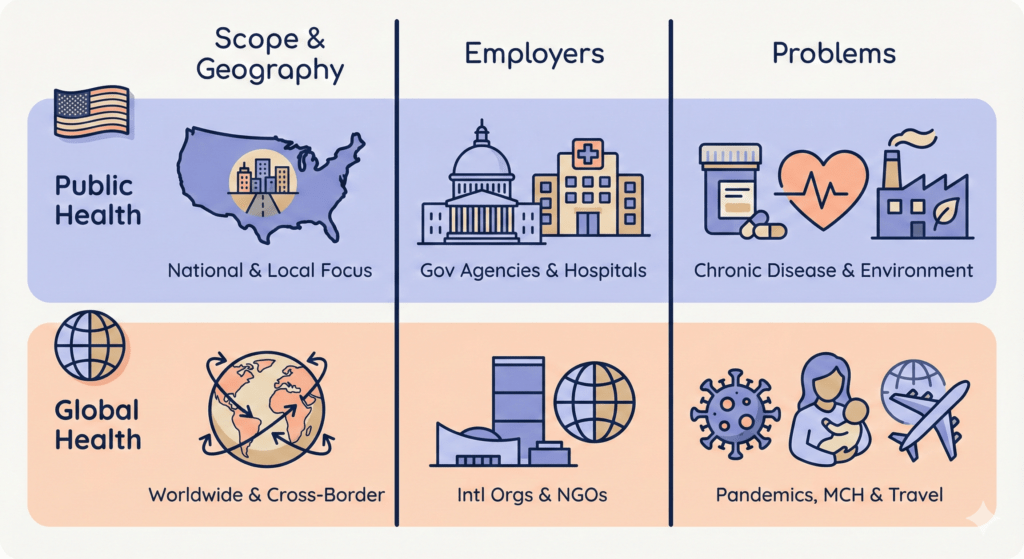
- Which employers immediately “get” your profile (US health departments and hospitals vs global NGOs and UN agencies). (ceph.org)
- Where the jobs actually are (the domestic public health workforce is large and structured; global health is more competitive and often tied to grants and foreign aid). (PMC)
- What kind of problems you’ll spend your career working on (US chronic disease, environmental health, and policy vs pandemics, health systems in low- and middle-income countries, humanitarian crises). (Encyclopedia Britannica)
This article is going to cut through the branding and answer three practical questions:
- What exactly is public health, and what does it look like in the US?
- What exactly is global health, and how is it genuinely different from public health?
- Given your goals, which degree label makes more sense – especially if you want to study and work in the United States?
By the end, you should be able to stop doom-scrolling program pages, pick a side (or a smart hybrid option like an MPH with Global Health concentration), and build a training path that actually matches the career you want.
Got it. Let’s redo that “quick comparison” section in a more natural, less robotic way.
Quick Comparison: How Global Health and Public Health Actually Differ
Before diving into details, it helps to answer one simple question:
Are you more interested in fixing health problems in your own system, or in working on issues that cut across countries?
That’s really the core split.
1. Where each field looks
- Public health usually zooms in on a specific population or country. In the US, that means cities, states, and national systems: Medicaid, CDC programs, local health departments, community clinics, school health, etc.
- Global health is built around health issues that don’t stop at borders: pandemics, migration, climate, conflict, and diseases that hit low- and middle-income countries hardest. The focus is on equity between countries as much as equity within a single country.
2. Who tends to hire you
In practice:
- With a public health profile in the US, you’re more likely to apply to:
- City or state health departments
- Federal agencies like CDC or HRSA
- Hospital systems, insurers, big US nonprofits
- With a global health angle, you’re looking more at:
- UN agencies (WHO, UNICEF, etc.)
- USAID and its implementing partners
- International NGOs and global health centers at universities
The skills overlap, but the organizations and day-to-day work culture can be very different.
3. What kinds of problems you’ll work on
Think in terms of day-to-day projects:
- Public health (US context) → designing a smoking-cessation campaign for one state, evaluating an obesity program in a school district, tracking opioid overdose trends, working on housing and environmental health in one city.
- Global health → supporting a TB program across multiple countries, helping a ministry of health rebuild services after conflict, working on vaccine rollout strategies for low-resource settings, or advising on global pandemic preparedness.
Same toolkit (epidemiology, data, program design). Very different playing field.
4. Typical degree labels
- If the program name has “Public Health” front and center (BSPH, MPH, DrPH), it’s usually pitched toward domestic systems, even if it offers global electives.
- If it uses “Global Health” in the title (Master of Global Health / Global Health Studies, or “MPH – Global Health”), it’s branding itself explicitly for cross-border work.
5. Rough rule of thumb
- If you imagine yourself working mostly in US cities, states, and national agencies, public health is the safer and clearer bet.
- If you picture yourself moving between countries, working with ministries of health, NGOs, or UN projects, then a global health-branded route (or an MPH with a serious global health concentration) lines up better.
What Is Public Health?
Core definition and mission
In plain language, public health is about keeping whole populations healthy, not just treating sick individuals one by one.
The CDC Foundation’s standard definition is: public health is “the science of protecting and improving the health of people and their communities” through promoting healthy lifestyles, researching disease and injury prevention, and detecting, preventing, and responding to infectious diseases. (cdcfoundation.org)
The American Public Health Association (APHA) phrases it slightly differently but with the same idea: public health promotes and protects the health of all people and their communities, aiming to give everyone a safe place to live, learn, work, and play. (American Public Health Association)
Key points buried in those official lines:
- The unit of care is a population, not an individual patient.
- The main tools are prevention, policy, systems, and environments, not stethoscopes and prescriptions.
- When public health succeeds, nothing dramatic happens: no outbreak, no water crisis, fewer people getting diabetes in the first place.
In the context of global health vs public health, this is the “domestic” side: how you design and run systems so that people in a particular place (say, the US) have clean water, safe food, vaccination coverage, decent air, and a functioning health system.
What public health work actually looks like in the US
Strip away the slogans and you get concrete, often unglamorous work.
Typical US public health work includes things like:
- Disease surveillance and outbreak control
Tracking influenza, COVID-19, measles, foodborne outbreaks or opioid overdoses, spotting patterns in the data, and deciding when and how to intervene. - Health promotion and behavior change
Designing campaigns on smoking cessation, safer sex, nutrition, physical activity, mental health, or vaccination; evaluating whether they actually changed behavior. - Environmental and occupational health
Monitoring air and water quality, industrial pollution, workplace safety, housing conditions, and climate-related risks; pushing for regulations and enforcement. - Policy and systems work
Analyzing how laws, insurance structures, and health-care delivery models affect health; writing briefs, lobbying for policies, and implementing programs at city, state, or federal level. - Data, analytics, and evaluation
Using biostatistics, epidemiology, and program evaluation methods to decide what works, what doesn’t, and where to put limited resources.
In terms of employers, US-trained public health professionals show up across:
- Local and state health departments and tribal health agencies
- Federal agencies like CDC, HRSA, FDA, NIH
- Hospitals and health systems (quality improvement, population health, infection prevention)
- Community-based organizations and national nonprofits
- Private sector and consulting (health analytics, policy consulting, pharma/biotech public health roles)
The US Bureau of Labor Statistics groups core roles like epidemiologists inside the public health universe and currently projects about 16% job growth for epidemiologists between 2024 and 2034, which is much faster than the average for all occupations. (Bureau of Labor Statistics)
So this isn’t a “soft” field with no market; it’s a real labor market anchored in government, health systems, and large nonprofits.
Public health degrees in the US
On the academic side, when US schools say “public health degree” they usually mean one of a few standard options:
- Undergraduate level
- BA/BS/BSPH in Public Health or Community Health
- Often gives broad exposure to population health, plus some basic methods and policy
- Graduate/professional level
- MPH (Master of Public Health) – the flagship professional degree
- MS in Epidemiology, Biostatistics, Environmental Health, etc.
- DrPH (practice-focused doctorate)
- PhD in Public Health disciplines (research-focused)
Traditionally, the MPH was built around five core disciplines: biostatistics, epidemiology, environmental health, health policy/administration, and social & behavioral sciences. (Wikipedia) Most US programs still cover these, but many have started reshaping the core curriculum to include things like systems thinking, leadership, communication, and equity in more explicit ways. (PMC)
Two things matter a lot if you’re thinking about studying public health in the US:
- Accreditation (CEPH)
- The Council on Education for Public Health (CEPH) is the main accrediting body for schools and programs of public health. (ceph.org)
- Many US employers, fellowships, and certifications quietly prefer or require degrees from CEPH-accredited programs.
- Program focus and concentration
- Even inside “public health,” you have to choose a lane: epi/biostats, policy, environmental, global health, health education, etc.
- This is where the “global health vs public health” distinction starts to show up: some MPH programs are clearly geared toward US domestic work, others offer a Global Health concentration (we’ll come back to that when we compare degrees).
Bottom line for this section: public health is the toolbox and career path for protecting the health of populations, usually within a defined place like the US.
What Is Global Health?
Core idea and definition
Global health is not just “public health in another country”.
The most widely cited definition (Koplan et al., The Lancet, 2009) calls global health:
“An area for study, research, and practice that places a priority on improving health and achieving equity in health for all people worldwide.”
Key pieces in that definition:
- “All people worldwide” → not limited to one country or region.
- “Equity” → it’s explicitly about unfair gaps in health between and within countries.
- “Transnational issues” → many problems (pandemics, climate, migration, trade, conflict) cross borders and can’t be solved by one country alone.
A recent systematic review makes the overlap with public health clear: both care about prevention, populations, and social determinants, but global health adds a stronger focus on global power, resources, and structural inequality.
So in practice:
- Public health asks: “How do we improve health in this system / this country?”
- Global health asks: “How do we reduce unfair health gaps across countries and deal with threats that affect everyone?”
What global health work actually looks like
Forget the Instagram version of “flying around saving the world”. Real global health work is usually structured, technical, and heavily project-driven.
Typical global health work includes:
- Large-scale infectious disease programs
- HIV, TB, malaria, and other high-burden infections in low- and middle-income countries.
- USAID, PEPFAR and partners funding treatment and prevention campaigns (e.g., antiretroviral access, malaria control).
- Pandemic preparedness and outbreak response
- Surveillance networks, lab systems, and rapid response teams across multiple countries.
- Recent investments like the Sentinel network in Africa show how global health now leans heavily on early-warning systems and local capacity, especially as traditional funding is cut.
- Health systems and policy in low-resource settings
- Working with ministries of health on financing, workforce, supply chains, and service delivery.
- Designing policies to expand primary care, maternal and child health, or non-communicable disease services.
- Humanitarian and conflict-related health work
- NGOs and UN agencies running or supporting health programs in conflict zones or during displacement, often under unstable conditions.
- Global health equity and governance
- Research and advocacy around who controls money, medicines, and data; how trade, patents, and geopolitics affect who gets care.
The workforce is spread across:
- Big bilateral funders (USAID, FCDO, etc.) and their contractors.
- UN agencies and global partnerships (WHO, UNICEF, Global Fund, Gavi).
- International and local NGOs delivering services on the ground.
- University global health centers doing research and technical support.
For a US-based student, this usually means you’re either:
- based in the US working on global projects with frequent travel, or
- posted in another country for months/years at a time, often through an NGO, university, or UN contract.
Global health degrees in the US
On program pages, you’ll see “global health” show up in three main ways:
- Standalone Master’s in Global Health
- Example: MS in Global Health at Georgetown, Duke, Boston University, etc.
- Usually emphasize:
- Global disease burden and health systems
- Quantitative + qualitative methods
- Ethics, equity, and power in global health
- Practice or thesis tied to an international project
- MPH with a Global Health concentration
- Many top US schools (Harvard, Hopkins, etc.) offer an MPH – Global Health track inside a standard MPH.
- You get:
- The classic MPH core (epi, biostatistics, policy, environmental, social & behavioral)
- Plus concentration courses on global health policy, health systems, humanitarian response, etc.
- This is often the most practical option if you want the MPH brand plus a clear global angle.
- Undergraduate majors/minors in Global Health / Global Public Health
- Many US universities now offer BA/BS programs in global health or “global public health”, framed around cross-border determinants, equity, and interdisciplinary approaches.
Curriculum themes you see repeatedly across these programs:
- Global burden of disease and comparative health systems
- Social, political, and economic determinants across countries
- Ethics, decolonizing/global power critiques
- Program design, monitoring and evaluation in low-resource settings
- Field placements or practicums with NGOs, ministries, or UN agencies
How this contrasts with “plain” public health
You already saw that public health is about populations, prevention, and systems. Global health uses the same core methods, but:
- Broadens the geographic lens: cross-border rather than mostly national.
- Puts equity between countries and regions front and center.
- Forces you to think about funding politics – e.g., what happens to programs and jobs when USAID or another big donor cuts money, which we’re seeing right now.
That’s why global health careers tend to be:
- more exposed to shifts in foreign aid and philanthropy,
- more competitive, and
- more dependent on grants and contracts than many domestic public health roles.
Key Differences: Global Health vs Public Health (In Practice)
You already know they overlap. Both care about populations, prevention, and equity. The real question is: where do they pull your career?
Think about these four angles.
1. Where your work is focused
- Public health is usually anchored in one system. In the US that means: states, cities, tribal nations, and federal programs. Your daily work is about improving health inside that system – e.g., how do we cut overdose deaths in this state, or improve maternal health in this county. (publichealthdegrees.org)
- Global health looks at problems that don’t care about borders: pandemics, migration, trade, climate, conflict, supply chains. The classic Koplan definition explicitly stresses “equity in health for all people worldwide” and “transnational health issues, determinants and solutions.” (PMC)
So:
- Public health = “fix this system, this population, this country.”
- Global health = “deal with inequities and threats that link many countries together.”
2. Who pays you and how stable it is
Public health (US-focused)
Typical employers:
- Local and state health departments
- Federal agencies like CDC, NIH, HRSA, FDA
- Hospital systems, insurers, big US nonprofits
- Health analytics and policy consulting shops (publichealthdegrees.org)
It’s not perfectly safe (US public health has had funding swings and layoffs, especially post-COVID), but overall it’s a large, structured workforce with clear job families: epidemiologist, program manager, policy analyst, infection preventionist, etc. (publichealthdegrees.org)
Global health
Typical employers:
- UN agencies (WHO, UNICEF, etc.)
- USAID and other donors, plus their implementing partners
- International NGOs and humanitarian organisations
- University global health centres and big foundations (News-Medical)
Here the money is more political and more fragile. When donors change priorities, projects end and contracts disappear. If you go this route, you’re implicitly accepting more volatility for the chance to work on cross-border issues.
3. The problems you actually spend time on
Public health – typical US projects:
- Tracking and reducing chronic diseases (diabetes, heart disease, cancer)
- Responding to opioid overdoses and substance use trends
- Dealing with environmental and occupational risks (air, water, housing, workplace safety)
- Designing and evaluating maternal, child, and mental health programmes in US communities
- Working on policy and systems: Medicaid, ACA implementation, local health equity work (publichealthdegrees.org)
Global health – typical project themes:
- HIV, TB, malaria, and other high-burden infections in low- and middle-income countries (News-Medical)
- Pandemic preparedness and outbreak response across regions
- Primary care, maternal and child health, and health-system reform in low-resource settings (PMC)
- Health in conflict and humanitarian crises
- Big structural issues: climate change, food insecurity, migration as health problems (PMC)
So ask yourself: do you see yourself buried in US Medicaid rules and local overdose data, or in Global Fund grants, WHO guidelines, and ministry-of-health meetings?
4. Same toolkit, different frame
Training-wise, the overlap is huge:
- Epidemiology
- Biostatistics
- Program design, monitoring and evaluation
- Health policy and systems
- Social and behavioural sciences (publichealthdegrees.org)
Global health usually layers on:
- Cross-cultural work and power dynamics
- Global governance, international law/policy
- Health systems in low- and middle-income countries
- Ethics and “decolonising” global health – who controls money, data, and decisions (PMC)
You’re not learning some magical new method set; you’re applying the same tools in messier, more unequal political environments.
5. Ruthless decision rule
Forget the branding for a second and answer honestly:
- If you want to live and build a long-term career mainly inside the US, with a relatively predictable market (health departments, hospitals, US agencies), then you should treat public health / MPH as your default, and add “global” via electives, a concentration, or specific projects.
- If you genuinely want to work across countries, you’re okay with donor politics and contracts that come and go, and you’re drawn to big North–South inequities and transnational threats, then a global health degree or an MPH with a serious global health track makes sense.
Degree Choices in the US – MPH vs Global Health Master’s vs Hybrid Options
Now we get to the part that actually shows up on your applications: what the degree is called and what that label quietly signals to US employers.
Think in three buckets:
- Classic MPH (Master of Public Health)
- Stand-alone Master’s in Global Health (MS/MA/MSc)
- MPH with a Global Health concentration/track
Plus a quick note on undergrad options at the end.
1. MPH: the default, and still the main “currency”
In the US, the MPH is the workhorse professional degree. Hopkins, Yale, BU, NYU, Columbia, etc. all run very similar structures:
- Core training in the five standard public health disciplines:
epidemiology, biostatistics, environmental health, health policy & management, and social/behavioral sciences. - Then a concentration (epi, policy, MCH, etc.), an applied practice/practicum, and some kind of integrative project, thesis, or capstone.
The Council on Education for Public Health (CEPH) sets the accreditation criteria for these programs and defines the foundational knowledge and competencies MPH grads are supposed to have. A CEPH-accredited MPH is basically a signal to US employers that:
- you’ve had a real core in methods, not just “global issues talk”, and
- you’ve done supervised field or practice work, not only classroom theory.
How it positions you
- Strong default for US health departments, CDC-type roles, hospitals, big US NGOs, and a lot of consulting roles.
- Also accepted for many global health jobs, if your practicum, electives, and experience are clearly global.
If you want maximum flexibility (domestic + some global), a CEPH-accredited MPH is still the safest bet.
2. Stand-alone Master’s in Global Health: sharper signal, narrower brand
These are degrees like MS/MA/MSc in Global Health at places like Northwestern, Duke, UCSF, IU, etc.
Look at their common patterns:
- Core blocks like: Foundations of Global Health, Global Disease Burden, Health Systems & Policy, Methods (quant + qual), and Global Determinants.
- A required practicum or field-based project, often 8–10+ weeks in a partner country or global program.
- Heavy emphasis on equity, social determinants, and cross-cultural work, sometimes blended with sustainable development, climate, or humanitarian themes.
This kind of degree screams: “I want to do global health, specifically.” That can help with:
- UN/NGO applications
- University global-health centers
- Donor-funded project roles
But there are trade-offs:
- Some US domestic employers (state health departments, hospital systems) understand “MPH” instantly, but need a second look at “MS in Global Health”.
- You’re somewhat locked into the global brand; if you pivot later to purely US state-level work, you may need to explain your training more.
If you are very clear that you’re chasing global health as your main lane, a solid Global Health master’s is defensible. Just don’t pretend it’s as broad a signal as “MPH” in the US market.
3. MPH with a Global Health concentration: the pragmatic middle
Many schools now offer the obvious hybrid: a standard MPH plus a named Global Health track.
Examples:
- Harvard’s MPH in Global Health (45 credits) – MPH core plus global health systems, policy, and leadership work.
- University of Washington MPH in Global Health – common MPH core, then global-health coursework, plus a practicum and thesis/capstone linked to global projects.
- Yale’s Global Health Concentration, which any MPH department can add on top of their main track.
- USF and Arizona MPH programs with Global Health/Global Health Practice concentrations focusing on low-resource settings, international policy, and MCH/nutrition.
What this combo buys you:
- The MPH label (which domestic US employers immediately understand),
- plus an official “Global Health” stamp on your transcript and practicum.
If you’re even slightly unsure whether you’ll stay global forever, this is often the smartest hedge:
- You can sell yourself as MPH-generalist for domestic roles.
- You can still pitch the global angle (fieldwork, electives, concentration) for international roles.
4. Undergraduate majors: early positioning, not the end point
At undergrad level, the US market has exploded with:
- Public Health majors (BA/BS/BSPH)
- Global Public Health / Global Health / Public Health–Global Health hybrids
Examples:
- NYU’s undergrad Global Public Health pathways.
- Cornell’s Global & Public Health Sciences major.
- University of Washington’s Public Health–Global Health BA/BS.
- UNC’s BSPH options including Community and Global Public Health.
- Maryland’s BS in Global Health, Boston College’s Global Public Health major.
Reality check:
- These undergrad degrees are useful foundations and can help you get entry-level jobs or research assistant roles.
- For a lot of serious policy, epi, or program posts (domestic or global), employers will still expect graduate training (usually an MPH, MS, or similar).
So if you’re at the undergrad stage, the key is not the exact major name, it’s:
- method skills you picked up (statistics, epi, programming, languages),
- what you did outside class (internships, RA work, field experience).
The grad-school label is what will matter later.
5. How to choose between these degree labels
Brutal but simple:
- You want the widest recognition in the US + flexibility to go domestic or global →
CEPH-accredited MPH, ideally with strong global options (concentration, practicum, electives). - You are absolutely sure you want a global-only identity and will chase NGOs/UN/donor work hard →
A good Master’s in Global Health or an MPH-Global Health from a credible school is fine. Just accept you’re tying your brand to that lane. - You’re early (undergrad) and not sure →
Don’t overthink the label. Get a solid public/global health or related major, build method skills and real experience, and keep the MPH vs Global Health master’s decision for later.
Careers and Salaries – Where Each Path Actually Takes You
You’re not studying this stuff for fun. You want to know: what jobs do people actually get, and what does the money look like?
I’ll keep it anchored in the US job market.

1. Public health careers in the US
This is where the volume is.
Typical roles for someone with an MPH or related public health degree:
- Epidemiologist – surveillance, outbreak investigation, data analysis for state/local health departments, CDC, hospitals, or research projects.
- Health services / program manager – running public health programs, community initiatives, or hospital-based population health projects.
- Health educator / community health worker / outreach coordinator – especially in community organisations and nonprofits.
- Environmental / occupational health specialist – monitoring and managing environmental risks, workplace safety, inspections.
- Health policy analyst – working on Medicaid, ACA implementation, state policy, or advocacy.
US Bureau of Labor Statistics (BLS) numbers (rounded, you don’t need fake precision):
- Epidemiologists
- Median annual pay is in the $80k range, with higher salaries in pharma/biotech and federal government, lower in small local agencies.
- Growth is projected to be much faster than average over the next decade.
- Medical and health services managers (many public health grads end up here after a few years’ experience)
- Median pay is roughly in the six-figure range (~$110k+).
- Job growth is also well above average, driven by aging population and system complexity.
- Health educators / community health workers
- Median salaries are lower (often in the $50–60k band), with big variation by employer and location.
- These roles are often entry-level stepping stones rather than end goals.
What matters more than the exact number:
- Public health offers a wide salary ladder: you can start in the $50–70k range and climb into management / director roles with six-figure compensation if you’re willing to move, specialise, and take responsibility for budgets and teams.
- The market is broad – thousands of city/county/state departments, hospital systems, payers, big NGOs, and consulting firms.
If your baseline goal is “solid, middle-class, stable career in health/workforce inside the US”, public health provides a very realistic path.
2. Global health careers (often US-based, globally focused)
Global health isn’t a single job title; it’s a cluster of roles spread across donors, NGOs, and universities. Common ones:
- Program officer / program manager (global health)
Managing donor-funded projects (HIV, TB, malaria, MCH, health systems, etc.): budgets, partners, reports, travel to field sites. - Monitoring, evaluation, and learning (MEL) specialist
Designing indicators, logframes, mixed-methods evaluations for projects across multiple countries. - Technical advisor / specialist
Deep expertise in a specific area (HIV, RMNCH, immunisation, health financing, humanitarian health) advising governments and NGO teams. - Global health researcher
At universities or research institutes, working on multi-country studies, implementation research, policy work. - Emergency / humanitarian health roles
Working with NGOs or UN agencies in conflict, disaster, or displacement settings.
On pay:
- US-based global health program officers / managers / advisors at big NGOs, UN agencies, or contractors often sit in roughly the same broad pay band as mid-level public health managers, frequently somewhere in the $70k–$120k+ range depending on organisation, seniority, and location.
- Some UN and major foundation roles can go higher, but they’re competitive and not entry-level.
- Field-based contracts (especially early humanitarian roles) can be decent but not spectacular when you factor in instability, time away from home, and short-term funding cycles.
The big difference is not the median salary – it’s how you get and keep the job:
- Jobs are often tied to specific grants and donor cycles. When a grant ends, your contract may end.
- Hiring can be network-driven: prior field experience, connections in specific NGOs/donors, languages, and niche expertise matter a lot.
- You may spend periods between contracts, move countries, or shift employers more often than a typical US state-health-department employee.
If you want impact + international exposure, this is the trade-off: more volatility for more global scope.
3. How employers read your degree label
Roughly how it lands in a hiring manager’s brain:
- MPH (general or standard concentration)
- “Good, they understand core methods and public health practice.”
- Strong fit for US domestic roles, still acceptable for global if backed by global experience.
- MPH, Global Health concentration
- “They have the standard MPH core plus explicit global training.”
- Flexible: works for US roles and for global project roles.
- Master’s in Global Health (non-MPH)
- “Clearly global health-oriented; need to check how strong their methods training is.”
- Strong signal for NGOs/UN/global research, but may require extra explanation for a random US health department job.
So if your priority is “I just want to be employable in a lot of places in the US”, the MPH label (ideally from a CEPH-accredited program) is still the safest currency.
If your priority is “I want my CV to scream GLOBAL HEALTH”, then a branded Global Health master’s or MPH-Global Health is fine – just know you’ll live and die more by global funding cycles and networks.
4. Matching path to your risk tolerance
Be honest with yourself:
- If you want predictability (clear ladders, pensions in some public roles, easier to switch states/cities), public health careers are the more rational bet.
- If you’re okay with contracts, grants ending, and moving when the money moves, and you get energy from working across countries and systems, global health can be worth the chaos.
Next in the article, you’d naturally move to a decision section: how to choose between global and public health based on where you want to live, what problems you care about, and how much volatility you’re actually willing to tolerate.
How to Decide: Global Health or Public Health?
This is the part where you stop “researching” and actually pick a lane.
You’re basically choosing between:
- Public health → Mostly domestic (US) systems, broader job market, more stability.
- Global health → Cross-border issues, more politics and travel, more competition and funding swings.
Use these filters one by one.
1. Where do you realistically want to live and work?
Not the fantasy version. The real one.
- If you see yourself:
- Living in US cities or states long term
- Working in health departments, hospitals, big US nonprofits, policy shops
- Maybe doing some international work later, but not as your core identity
- If you honestly want:
- Multi-country work as a default, not a side quest
- Long stretches in low- and middle-income countries
- Jobs tied to donors, UN agencies, or large NGOs
If your answer is “I don’t know, maybe both” → you’re not a special case; you’re exactly the normal case. That’s what the MPH with Global Health concentration is for.
2. Which problems piss you off the most?
Look at what actually bothers you when you read the news or papers.
- If it’s:
- US health insurance chaos
- Racial and socioeconomic disparities inside the US
- Opioid crisis, gun violence, mental health access
- Local water, housing, and environmental injustice
- If it’s:
- Why some countries still don’t have reliable access to basic vaccines or antibiotics
- How climate, debt, trade, patents, and colonial history shape who lives and dies
- Pandemic failures across borders, not just in one system
- Wars, displacement, famine, and global funding politics
Your degree should point toward the cluster of problems that actually keep your brain spinning at 2 a.m.
3. How much chaos are you willing to tolerate in your career?
Be brutally honest:
- Lower chaos tolerance
- You like clear ladders, permanent roles, and know roughly what you’ll earn next year.
- You’re fine with bureaucracy as long as the paycheck is predictable.
- Higher chaos tolerance
- You can live with funding cycles, contracts, and projects that end.
- You’re okay moving cities/countries or organisations when grants die.
- You don’t panic at the idea of “we have funding for 2–3 years; after that, we’ll see.”
You can absolutely have global work with an MPH, but the more you lock yourself into a pure global brand, the more exposed you are to donor mood swings.
4. What’s your plan B if the ideal job doesn’t show up?
You need a fallback.
- With a CEPH-accredited MPH, plan B is relatively forgiving:
- Local/state health departments
- Hospital/health system roles
- Nonprofits, consulting, policy shops
- You can still chase global fellowships, NGOs, and UN projects later if you build experience.
- With a pure Global Health master’s, plan B is narrower:
- You’re mainly playing in the same global/donor/NGO space.
- Pivoting to random US state-level roles is possible, but you’ll be explaining your degree more and may need stronger methods/language on your CV to compensate.
If you’re not the type who enjoys constantly hustling for the next niche grant-funded job, don’t pretend you are.
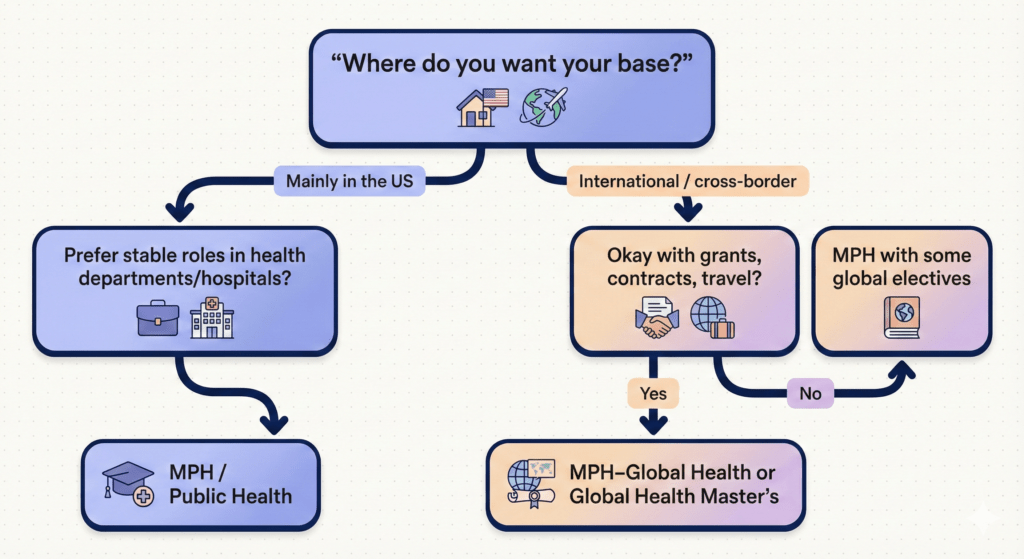
5. A simple decision tree
Use this as a sanity check:
- Do you want your core career base to be inside the US?
- Yes → Go MPH (public health). Add Global Health concentration if you still want international exposure.
- No / Not really, I want to move around internationally → Go to question 2.
- Are you okay with grant cycles, contracts, and sometimes unstable postings?
- Yes → A strong Global Health master’s or MPH–Global Health is reasonable.
- No → You want global flavor without global risk. Stick to MPH and build global experience via practica, fellowships, and employers with international portfolios.
- Are you still completely torn?
- Choose a CEPH-accredited MPH at a school with a serious Global Health track.
- Load your electives, practicum, and thesis with global content.
- If later you decide you’re done with global, you still have a standard MPH that domestic employers instantly understand.
6. What you should actually do next
If you’re serious about this and not just passively reading articles:
- Make a 2-column list:
- Column A: “US public health problems I care about”
- Column B: “Global / cross-border problems I care about”
See which column fills faster and with more emotion.
- Grab 5–10 programs and classify them:
- MPH (domestic oriented)
- MPH – Global Health
- Master’s in Global Health
Look at: - CEPH accreditation
- Practicum/field options
- Where alumni actually work (not marketing slides, real LinkedIn stalking).
- Decide your risk level (low / medium / high) and pick the degree label that matches it.
FAQs – Global Health vs Public Health
Let’s clean up the most common doubts people still have after reading everything above.
1. Is global health the same as public health?
No.
They share the same core toolkit (epi, biostats, policy, systems, social determinants), but they don’t frame the work the same way:
- Public health → protects and improves health in a defined population, usually within a single country (for you, think US states, cities, and national systems).
- Global health → looks at health across countries, focusing on transnational issues and on inequities between and within countries (“equity in health for all people worldwide” is the classic phrasing).
Overlap is big, but the geography, politics, and day-to-day problems are different.
2. Is global health just “public health somewhere else”?
That’s the lazy definition. It’s also exactly what a lot of people in the field argue against.
The more serious view:
- Global health is not only about “going abroad”. It is about how power, money, trade, patents, aid, and history create health gaps between countries.
- It forces you to deal with donor politics, colonial legacies, global governance (WHO, World Bank, WTO, etc.), and structural stuff you rarely touch if you stay purely in a US domestic lane.
So “public health somewhere else” is incomplete at best. You can use that as a quick analogy for a layperson, but if that’s how you actually think about it, you’ve missed half the point.
3. Which is better if I want to work at CDC or in a US health department?
For CDC, NIH, FDA, HRSA, and state/local health departments, the safest, clearest option is:
- MPH (standard public health degree) from a CEPH-accredited program, with a relevant concentration (epi, health policy, environmental health, MCH, etc.).
You can absolutely add a Global Health concentration or global electives and still be fine. But if your main goal is US government or state/local roles, do not over-optimize for a fancy “Global Health” label and undercut your core methods training.
4. Which is better if I want to work for WHO, UNICEF, or big global NGOs?
Here the branding and experience matter more:
- A Global Health master’s or an MPH with a strong Global Health track helps because:
- your coursework matches the themes they care about;
- your practicum/thesis can be tied to their type of projects.
BUT:
- They care at least as much about your field experience, languages, and networks as about what’s printed on the diploma.
- A rock-solid MPH + serious global fieldwork + languages + good references can compete just fine with a pure Global Health degree.
So: if your entire life plan is WHO / UNICEF / global NGOs, don’t be scared of “Global Health” branding – just don’t rely on the label alone to carry you.
5. Can I move from public health to global health later (or vice versa)?
Yes, but you pay in time and effort.
- Moving from public → global
- Easiest path: MPH or public-health degree, then build global experience via:
- global practicum/fellowships
- working for NGOs or universities on international projects
- languages + time in the field
- Many global health people started as “plain” public health professionals.
- Easiest path: MPH or public-health degree, then build global experience via:
- Moving from global → domestic US public health
- Also doable, but some domestic employers will need reassurance you have:
- strong methods skills
- understanding of US systems
- ability to apply your experience to domestic issues
- Also doable, but some domestic employers will need reassurance you have:
The underlying skill set is transferable. What takes time is switching networks and proving relevance in the new space.
6. Does a Global Health master’s limit me if I decide I don’t want to work internationally anymore?
It can, depending on how you use it.
- If the degree is light on methods and heavy on “global issues talk”, some US employers (especially technical ones) will see you as under-tooled.
- If you’ve taken strong epi/biostats/policy methods and can show applied work (even if global), it’s much easier to pivot.
This is why the MPH with Global Health concentration is a safer hedge if you’re not 100% committed to global forever.
7. Do I need a PhD or DrPH for either path?
Most people do not.
You consider a doctorate if:
- You want to be faculty / PI / high-level researcher.
- You’re aiming at very senior policy or technical roles where a doctorate is either expected or a big advantage.
For the majority of practitioner roles (epi, program management, MEL, technical advisor, etc.), a good MPH or Global Health master’s + solid experience matters more than collecting extra degrees.
8. As an international student, should I still pick public vs global the same way?
Yes, logic is the same; only your constraints differ:
- Visa issues, work authorization, and funding may push you toward particular countries or employers.
- You should still ask:
- Where do I want to build my base?
- Am I aiming for US domestic work, global work, or both?
- Which degree label will be easiest to explain in my home country + the US + any third country I might target?
In many cases, an MPH with a Global Health focus is still the most portable pick.
9. Is one path “more impactful” than the other?
No. That’s ego talking.
- You can waste your life in both global and domestic roles doing pointless box-ticking.
- You can also do serious, high-impact work in both, depending on the team, the problem, and how honest your organisation is about results.
The only real question is: Which problems and settings do you care enough about to stay in the fight when it gets boring, bureaucratic, or political?
Internal Links:
CEPH-Accredited MPH Programs (2025 Guide)
CEPH-Accredited MPH Programs in New York (2025)
Accelerated 1-Year MPH Programs (2025 Guide): Accredited 12-Month MPH Options
MPH vs MHA vs MBA (2025): Which Health Degree Is Best for You?
