If you’re comparing MPH vs MSPH vs MHS and trying to decide which public health master’s degree fits your future, you’re not alone. These three programs look similar on paper, but they prepare you for very different careers in practice, research, and specialized health science.Table of Contents
Quick Answer: MPH vs MSPH vs MHS
An MPH is usually the best choice if you want a practical public health career in program management, epidemiology, health policy, community health, global health, or applied public health leadership. An MSPH is usually more research-heavy and fits students who want stronger methods training, a thesis-style experience, or a path toward doctoral study. An MHS is usually more specialized and depends heavily on the department offering it.
| Degree | Best for | Usually emphasizes |
|---|---|---|
| MPH | Applied public health careers | Practice, leadership, fieldwork, and population-health problem solving |
| MSPH | Research-focused public health students | Methods, analysis, research design, thesis or master's essay work |
| MHS | Specialized health science paths | Department-specific technical training, policy, research, or applied health science |
What does MSPH mean?
MSPH means Master of Science in Public Health. Compared with an MPH, it normally signals a stronger research or methods orientation, though exact requirements vary by university.
What does MHS mean?
MHS usually means Master of Health Science. It is less standardized than the MPH, so the right question is not just "MHS vs MPH" but what department, concentration, thesis option, and career path the specific MHS is built around.
MPH vs MSPH: which is better?
Neither is universally better. Choose the MPH if you want broad applied public health training. Choose the MSPH if you want deeper research preparation or are considering a PhD, DrPH, or analytics-heavy role.
If you are still building a school list, start with the Best MPH Programs guide, then compare online MPH options, no-GRE MPH programs, and CEPH-accredited MPH programs.
Introduction
If you’ve started exploring graduate options in public health, you’ve probably run into three very similar-sounding degrees: MPH, MSPH, and MHS. On paper they all sit in the same universe. In reality, they can lead you toward very different kinds of work and very different expectations in grad school. Research.com
In simple terms:
- The MPH (Master of Public Health) is built for hands-on public health practice and leadership – the people who run programs, design interventions, and work with communities and health systems. Wikipedia
- The MSPH (Master of Science in Public Health) leans into research and analytics – the people who design studies, crunch data, and publish evidence to guide policy and practice. Research.com
- The MHS (Master of Health Science) is usually a specialized, technical master’s – often more narrowly focused on a specific field like epidemiology, global health, or health policy. publichealthdegrees.org+1
The problem is that universities don’t always make these boundaries crystal clear. Different schools use the titles differently, and blogs or forums often mix them up. So students end up asking the same questions over and over:
- “Is MSPH higher than MPH?”
- “Is MHS just another name for MPH?”
- “Which one actually helps me get the job I want in the US?” Research.com+1
This guide is written for future students who want to study or work in public health in the United States – whether you’re:
- finishing a bachelor’s and thinking about grad school,
- already working in health and considering a career move, or
- aiming long-term for a PhD/DrPH, research career, or leadership role in public health.
Over the rest of this article, we’ll break down, side by side, how the MPH, MSPH, and MHS differ in:
- focus (practice vs research vs specialization),
- curriculum and workload,
- thesis vs practicum expectations, and
- career outcomes and salaries in the US. Research.com+1
By the end, you should be able to answer one question honestly for yourself:
“Given the kind of work I want to do in public health, which degree is actually the right tool for me – MPH, MSPH, or MHS?”
What Each Degree Actually Means (Without the Marketing Spin)
Let’s stop treating these three as mysterious acronyms and call them what they really are in terms of purpose and design.
1. Master of Public Health (MPH) – The Professional Practice Workhorse
What it is:
The MPH is the standard professional master’s in public health practice. It’s designed to prepare you to work in the field – health departments, NGOs, hospitals, international agencies – not to sit in a lab running regression models all day. (Wikipedia)
Typical MPH programs in the US:
- Are broad and generalist, covering the main public health disciplines:
epidemiology, biostatistics, environmental health, health policy/management, and social & behavioral sciences. (Wikipedia) - Include a practicum, internship, or field-based capstone where you apply what you’ve learned in a real-world setting. (University of San Diego Online Degrees)
- Emphasize program design, implementation, and leadership, not just theory.
At places like Johns Hopkins, the MPH is explicitly described as a broad-based, school-wide degree that prepares students to work on diverse public health issues, and often requires prior health-related work experience. (JHU Bloomberg School of Public Health)
What the MPH signals to employers (in the US):
“This person has a broad, applied public health skill set and can work on real programs, policies, and interventions.”
If you want to run programs, manage teams, work in government, NGOs, or health systems, and you care more about impact in the field than about publishing papers, MPH is built for that.
2. Master of Science in Public Health (MSPH) – The Public Health Research Track
What it is:
The MSPH is a science-heavy, research-oriented public health master’s. It still lives in the public health world, but its center of gravity is methods, data, and research, not day-to-day program operations. (Healthcare Management Degree Guide)
Compared with a typical MPH, MSPH programs:
- Cover the same core public health areas (epi, biostats, policy, environmental, social/behavioral) but go deeper into research methods, quantitative analysis, and sometimes health informatics. (University of San Diego Online Degrees)
- Nearly always require a thesis or substantial research project, not just a practicum or capstone. (University of San Diego Online Degrees)
- Expect graduates to be able to design studies, analyze data, and critically evaluate evidence, not just “use” public health research.
At Johns Hopkins and similar schools, MSPH is often positioned as a department-based degree for students who want more focused skills in a specific area of public health, and in some departments it’s the option for those without the 2 years of health-related work experience required for the MPH. (JHU Bloomberg School of Public Health)
What the MSPH signals to employers and PhD committees:
“This person is comfortable with data, methods, and research, and can contribute to the design and analysis of public health studies.”
If your long-term plan is PhD/DrPH, academic research, epidemiology, biostatistics, or data-heavy roles (e.g., research analyst, public health scientist), MSPH is usually a better fit than a generic MPH.
3. Master of Health Science (MHS) – The Specialized / Flexible Option
What it is:
The MHS (or MHSc) is a specialized health science master’s, and it’s more flexible as a category than MPH or MSPH. Depending on the school and department, an MHS can be:
- Research-oriented, giving you advanced training in methods and a thesis;
- Professionally oriented, focused on applied skills in a specific health area. (Wikipedia)
Core reality: MHS is not one standard model. Each institution designs it differently.
Examples:
- At Johns Hopkins, there are multiple MHS tracks inside departments (Biostatistics, Mental Health, Population/Family/Reproductive Health, Global Health Economics, etc.), each with its own structure and goals. (JHU Bloomberg School of Public Health)
- Many MHS programs are more specialized than an MPH, often focusing on a narrow area like environmental health, health economics, or specific population groups. (publichealthdegrees.org)
- Some MHS programs are explicitly designed to provide strong clinical or research methodology skills, especially for clinicians who want to do research. (UBC Grad School)
What the MHS signals to employers/academia:
“This person has focused, technical training in a specific health science or public health subfield.”
MHS can work well if:
- You already know your exact niche (e.g., global health economics, environmental health, biostats);
- You want strong methods or technical skills without doing a generic public health generalist degree;
- You’re using it as a bridge to research careers or further postgraduate training. (Research.com)
Snapshot: How to Think About Them in One Line
- MPH → Broad professional public health practice degree.
- MSPH → Research-focused public health science degree.
- MHS → Specialized health science/public health degree whose exact flavor depends heavily on the school and department.
Side-by-Side Comparison: MPH vs MSPH vs MHS
You don’t choose a degree based on vibes. You choose it based on structure, workload, and where it actually lands you. Here’s the fast, side-by-side answer most people are really looking for when they Google “MPH vs MSPH vs MHS”.
1. Quick Comparison Table – MPH vs MSPH vs MHS
| Dimension | MPH | MSPH | MHS |
|---|---|---|---|
| Type of degree | Professional practice degree in public health | Academic / science-oriented public health degree | Specialized health science / public health degree |
| Primary focus | Broad public health practice, programs, policy, community work | Research methods, epidemiology, biostatistics, data & evidence | Narrower specialization (e.g. epi, global health, health economics, environmental health) |
| Orientation | Generalist, applied | Analytical, research-heavy | Specialized (can be research- or practice-leaning depending on school) |
| Core curriculum | Public health fundamentals (epi, biostats, env health, policy, social & behavioral) + practicum/capstone | Same core areas but with deeper methods, stats, and research design + thesis/practicum | Varies a lot by program; usually concentrated in one subfield with supporting methods courses |
| Practicum / fieldwork | Common and usually required (internship / practicum / applied capstone) | Often includes practicum plus extended research or thesis | Depends on program: some have practica, some are purely coursework + project/thesis |
| Thesis expectation | Often no formal thesis; capstone or project instead | Thesis or substantial research project is standard | Mixed: some are thesis-based, some are project-based, some mostly coursework |
| Typical duration (full-time) | ~2 years in many US programs (some 1-year intensive formats) | ~2 years is common; some programs structure it as 2 years with long field placement | 1–2 years depending on department and specialization |
| Entry profile | Often prefer or require health-related work experience at top schools | More open to students straight from undergrad, especially if strong in quantitative work | Varies widely; some target clinicians or working professionals, others accept fresh grads |
| Ideal for | People who want to work in the field: health departments, NGOs, hospitals, global health programs, implementation | People who want to do research, pursue a PhD/DrPH, or work in data-heavy roles (epi/biostats/policy research) | People who already know their niche and want focused technical training in that area |
| How employers read it (in practice) | “Ready for frontline public health practice and program roles.” | “Comfortable with research methods and data; good fit for research/analytic posts and PhD track.” | “Has specialized training in X area; strength depends heavily on the specific program and school.” |
This table is synthesized from reputable program descriptions and comparisons from Johns Hopkins, publichealthdegrees.org, Coursera, and other US-based academic sources. (JHU Bloomberg School of Public Health)
2. How to Read This (So You Don’t Overthink It)
a) Practice vs Research vs Specialization
If you strip away all branding:
- MPH → built for practice (running programs, managing interventions, working in systems). (Masters Public Health)
- MSPH → built for research and methods (designing studies, running analyses, publishing evidence). (University of San Diego Online Degrees)
- MHS → built for focused expertise in a particular area (and its exact flavor depends heavily on the department/school). (publichealthdegrees.org)
When you don’t yet know your niche and just “want to do public health,” you’re usually in MPH territory.
On the other hand, students who already enjoy stats, epi, methods and numbers generally find that MSPH fits better.
Finally, anyone who is clear from the start — “I want health economics” or “I want environmental epi only” — will often get more value from an MHS focused on that niche.
b) Practicum vs Thesis – What Your Day-to-Day Looks Like
- MPH = you’ll spend serious time doing fieldwork / practicum / capstone with a real organization. It’s built into how the degree proves you’re “practice ready.” (University of San Diego Online Degrees)
- MSPH = you’ll still get practice exposure, but the degree usually expects a thesis or substantial research project on top, and significantly more quantitative coursework. (JHU Bloomberg School of Public Health)
- MHS = the structure is all over the map; some are pure clinical or research methods (e.g., clinical research MHS), some look like mini-MPHs in a niche. You cannot assume anything without reading that program’s page line by line. (Wikipedia)
So if the idea of a formal thesis makes you want to drop out before you even start, MSPH or thesis-based MHS may not be your best friend.
c) Flexibility for Future Study (PhD / DrPH)
Reality check:
- An MPH can still get you into a PhD/DrPH, but you’ll need to prove you can handle methods and research. It’s often seen as a terminal professional degree. (edX)
- An MSPH is basically marketing itself as “I’m serious about research” – PhD committees know this. (University of San Diego Online Degrees)
- An MHS can be excellent for PhD entry if it’s research-heavy and recognized at that institution (e.g., Hopkins/Yale-style research MHS). But again, it depends entirely on the program design. (publichealthdegrees.org)
If your non-negotiable is “I want to do a PhD in epi/biostats/public health,” you should be leaning MSPH or a clearly research-oriented MHS, not a generic MPH with minimal methods.
d) Employer Perception (US Context)
Most US employers in public health aren’t obsessing over the exact letters; they care about:
- What skills you actually have (methods vs program management vs policy vs niche expertise)
- What you did (thesis topic, practicum site, projects, previous work) (Research.com)
But as a rough rule of thumb:
- MPH = “day-one useful in programs and practice.”
- MSPH = “plug into research / analysis roles quickly.”
- MHS = “specialist – depends what they specialized in and where.”
What You Actually Study (Curriculum & Structure Differences)
Now let’s stop talking in abstractions and look at what your day-to-day academic life actually looks like in each degree.
1. MPH – Broad Core + Practicum (Applied Practice Engine)
Most US MPH programs follow a similar logic:
- Foundational public health core
- Concentration/electives
- Practicum (applied experience)
- Capstone or integrative project
a) Core Curriculum
A typical MPH core will hit all the “classic” public health pillars:
- Epidemiology
- Biostatistics (basic to intermediate)
- Environmental and occupational health
- Health policy and management
- Social and behavioral sciences / health promotion
- Cross-cutting skills (communication, leadership, ethics, sometimes informatics) (JHU Bloomberg School of Public Health)
Example: Johns Hopkins lists its MPH core as grounding students in biostatistics, epidemiology, social and behavioral determinants, management sciences, problem-solving, demography, environmental health, biological sciences, and policy. (JHU Bloomberg School of Public Health)
Bottom line: MPH gives you breadth across the field, not obsessive depth in one narrow area.
b) Practicum / Applied Practice
This is where MPH clearly differentiates itself.
US MPH programs accredited under CEPH must provide practice-based training – basically, you don’t graduate without working in a real public health setting. (web.sph.uth.edu)
Examples from real schools:
- Johns Hopkins: minimum 100 hours of practicum experience plus a capstone project. (JHU Bloomberg School of Public Health)
- University of Chicago: applied practice experience, minimum 80 hours in a public health or related organization. (publichealth.bsd.uchicago.edu)
- Many US programs (Liberty, Iowa, Washington) require 120–200+ hours of structured fieldwork with defined deliverables. (public-health.uiowa.edu)
You’re not just shadowing; you’re supposed to produce something tangible: needs assessment, evaluation plan, policy brief, data report, toolkit, etc.
Translation: in an MPH, a serious chunk of your time goes into working with an actual organization, not just passing exams.
c) Capstone / Integrative Project
Most MPH programs end with a capstone instead of a classic thesis:
- You take what you’ve learned from coursework + practicum
- You apply it to a defined public health problem
- You produce a report, presentation, or product that shows you can integrate knowledge in a practical way (JHU Bloomberg School of Public Health)
If you want structured field experience and applied problem-solving as a core part of your training, this is exactly what MPH is designed to deliver.
2. MSPH – Heavier Methods, Field Placement + Master’s Essay
MSPH lives in the same universe as MPH but is noticeably more academic and research-heavy.
a) Core + Concentration
MSPH programs usually:
- Cover public health fundamentals (epi, biostats, policy, environment, social/behavioral) like an MPH
- Then push deeper into:
- Advanced epidemiologic methods
- Statistical modeling / analysis
- Research design, measurement, evaluation
- Specialized content (health systems, global health, nutrition, etc.) (JHU Bloomberg School of Public Health)
At Johns Hopkins, MSPH degrees are department-based — e.g., Health Systems, Global Disease Epidemiology and Control, Human Nutrition, Social and Behavioral Interventions — each with its own detailed curriculum and methods focus. (JHU Bloomberg School of Public Health)
So instead of “general public health + a bit of everything,” you’re doing public health in a specific domain with serious research tools.
b) Field Placement (Yes, Many MSPH Programs Still Do Practice)
People assume MSPH = only lab and Stata. Not true.
Many MSPH programs require both:
- A field placement (sometimes 4+ months full-time), and
- A substantial written project (often called a master’s essay). (JHU Bloomberg School of Public Health)
Example: Johns Hopkins MSPH in Population, Family and Reproductive Health:
- Minimum two terms (~4 months) full-time field work (at least 680 hours)
- Culminating master’s essay that integrates coursework + field experience (JHU Bloomberg School of Public Health)
So you do get real-world exposure, but it’s tightly tied to your research or analytic focus.
c) Master’s Essay / Thesis
Unlike the typical MPH capstone, MSPH almost always expects a research-style written product:
- Structured like a thesis or extended research paper
- Uses real data or systematic methods
- Supervised by faculty and often linked to your field placement or department research priorities (JHU Bloomberg School of Public Health)
If you want to publish, apply for research jobs, or position yourself for a PhD, this structure is a lot more attractive than a generic project report.
Net effect: MSPH gives you a hybrid profile – you’ve done both fieldwork and real research, with a methods-heavy curriculum to back it.
3. MHS – Program-Dependent but Usually Narrower and More Technical
MHS (or MHSc) is not standardized the way MPH is. The curriculum is heavily program-specific.
a) Core Pattern
Typical patterns you see in MHS programs:
- A health science core (legal, ethical, managerial, and public health aspects of healthcare), plus
- A specialized track (e.g., public health concentration, leadership, education, research). (Fairleigh Dickinson University)
Example: Fairleigh Dickinson’s MHS in Health Science:
- All students complete a health science core (legal, ethical, managerial, public-health issues)
- Then choose a track, which shapes the specific courses and focus. (Fairleigh Dickinson University)
Other MHS programs (especially those linked to public health schools) may offer:
- Clinical research methods
- Occupational and environmental hygiene
- Epidemiology or biostats specializations
- Public health concentration aligned with CEPH standards (CDC Stacks)
So MHS can be practice-leaning or research-leaning, but almost always narrower in thematic focus than a general MPH.
b) Thesis / Project vs Coursework
The structure here is variable:
- Some MHS programs are thesis-based, acting like a mini-MS for people wanting research training
- Others use a capstone or applied project, especially when focused on leadership/administration rather than hardcore methods
You cannot assume an MHS includes a practicum or a thesis — you have to read that specific program’s page.
c) What This Means for Your Weekly Life
Compared to MPH/MSPH:
- You’ll often take fewer “public health generalist” classes
- You’ll spend more time on one thematic area (e.g., health science core + your specialization) (Fairleigh Dickinson University)
- Practice vs research exposure will depend entirely on how the program is built
For someone who already knows “I want advanced training in X niche”, the MHS structure can be efficient. For someone still figuring out what they want, it can feel too narrow.
4. Practical Takeaways From the Curriculum Differences
If you strip out all the university marketing and look purely at what you actually do:
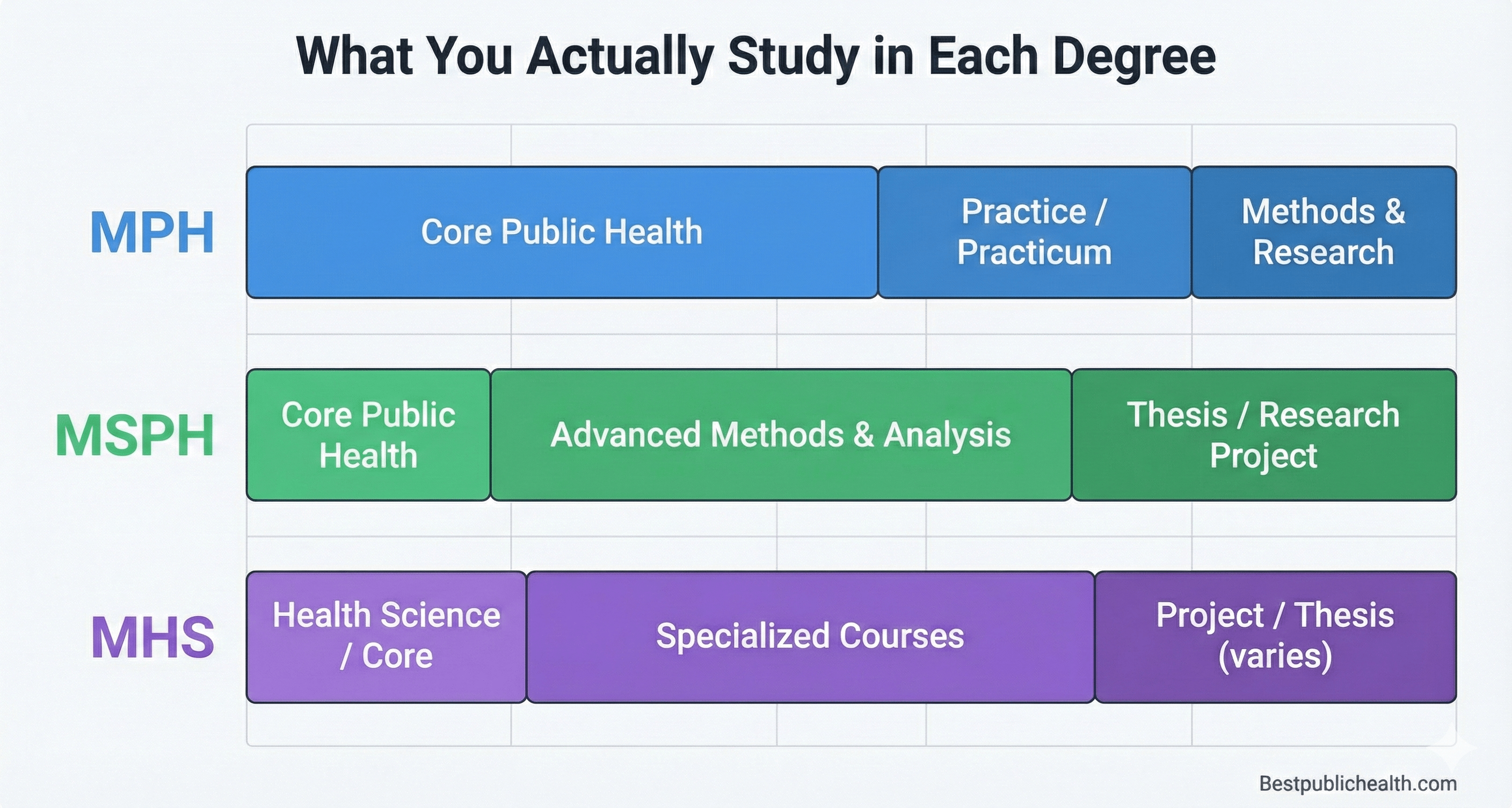
- In an MPH, you:
- Take broad core courses
- Choose a concentration
- Spend mandatory hours in a practicum
- Finish with a practice-oriented project/capstone (JHU Bloomberg School of Public Health)
- In an MSPH, you:
- Take focused, often more quantitative coursework in a specific public health domain
- Do a longer or more structured field placement
- Produce a thesis/essay-level research product (JHU Bloomberg School of Public Health)
- In an MHS, you:
- Follow a health-science or public-health core
- Go deeper into one track (e.g., public health, research, administration, education)
- May or may not do a practicum or thesis, depending on the design (Fairleigh Dickinson University)
So before you pick a degree label, you should be asking:
“What will my actual timetable, assignments, practicum, and final project look like in this specific program?”
Who Should Choose What? (Brutally Simple Degree–Person Match)
This is the part you actually care about:
Given the kind of person you are and the work you want to do, which degree makes sense – MPH, MSPH, or MHS?
I’m not going to give you the diplomatic “all are great” answer. Here’s the real mapping.
1. If You Want To Work In the Field → You’re an MPH Person
You should lean MPH if most of these are true:
- You want to work in health departments, NGOs, hospitals, community orgs, UN/INGOs. (publichealthdegrees.org)
- You like the idea of designing and running programs, not just analyzing data about them.
- You want applied skills: program planning, monitoring & evaluation, health promotion, policy implementation.
- You like real-world work: site visits, stakeholder meetings, working with communities, not just sitting behind a screen.
- You see this as a terminal professional degree – you’re not obsessed with doing a PhD. (edX)
Why MPH fits:
- It’s explicitly described as the professional practice degree in public health – broad, applied, and designed for workforce readiness. (Healthcare Management Degree Guide)
- Employers in US public health practice (local/state health departments, NGOs) typically recognize MPH as the standard qualification. (publichealthdegrees.org)
If your mental picture of “success” is leading programs and fixing real health problems in actual communities, stop overcomplicating it: MPH is your default.
2. If You Want a PhD / Research Career → You’re an MSPH Person
You should lean MSPH if this sounds like you:
- You enjoy stats, methods, and analytical work more than “community organizing”.
- You’re considering or already planning a PhD or DrPH, especially in epi, biostats, or health services research. (Research.com)
- You actually like the idea of a thesis, research design, and writing long papers.
- You want to be the one who designs studies, runs models, and publishes evidence, not just “uses” research someone else did.
Why MSPH fits:
- It’s consistently defined as the academic / research-oriented public health master’s that prepares people for doctoral study and research roles. (Research.com)
- Curriculum is more methods-heavy (advanced epi, biostats, research design, data analysis). (University of San Diego Online Degrees)
- Many MSPH programs require a substantial thesis or master’s essay plus extended field placement, which looks good on PhD applications. (JHU Bloomberg School of Public Health)
If your endgame is “I want to be a researcher / epidemiologist / academic”, doing a generic practice-focused MPH is an inefficient path. MSPH (or a clearly research-heavy MHS) is better aligned with that plan.
3. If You Already Know Your Niche → You’re Likely an MHS Person
You should seriously consider MHS if:
- You already know your exact niche (e.g., global health economics, mental health, environmental health, clinical research).
- You care less about broad generalist MPH content and more about deep skills in one focused area.
- You want a degree that’s either:
- research-oriented in that niche, or
- professionally targeted to a specific type of role. (publichealthdegrees.org)
What MHS actually is:
- A specialized master’s that can be academic or professional depending on the department.
- Often designed to give advanced study and research training in a specific public health/health science area, or to advance careers as public health professionals with focused skills. (Wikipedia)
Reality check: MHS is more program-dependent than MPH/MSPH:
- Some MHS programs function like mini research degrees.
- Some are professionally oriented with leadership/management focus.
So if you pick MHS, you don’t just pick the degree; you pick a very specific program whose structure and reputation matter a lot.
4. Work Experience vs Fresh Grad: Another Brutal Filter
This is often ignored but matters in the US:
- At Johns Hopkins and similar schools, the MPH is broad-based and usually requires 2 years of health-related work experience, whereas the MSPH is department-based and designed for people without that work history who want to begin a career in public health. (JHU Bloomberg School of Public Health)
So:
- If you’re a fresh graduate with limited experience and want structured, methods-heavy training → MSPH/MHS may be more accessible.
- If you’re already working in health/public health and want a credential to move into leadership or higher-responsibility practice roles → MPH fits your profile.
5. Simplified Decision Matrix (Stop Overthinking)
Ask yourself three questions:
- Do I want to be a practitioner, a researcher, or a niche specialist?
- Practitioner → MPH
- Researcher / future PhD → MSPH
- Niche specialist (and I know the niche) → MHS (or MSPH in that field)
- Do I want a practicum-heavy or thesis-heavy experience?
- Practicum-heavy, applied capstone → mostly MPH. (publichealthdegrees.org)
- Thesis-heavy, methods and data → mostly MSPH or research-style MHS. (publichealthdegrees.org)
- Is my non-negotiable goal a PhD/DrPH?
- Yes → design backward from PhD expectations (strong methods + thesis). That usually means MSPH or a solid research MHS.
- No → pick the degree that best matches your actual job target, not ego or letters.
Career Outcomes & Salary Patterns (By Degree Type)
I’ll be blunt: employers don’t care about your letters as much as they care about what you can actually do. But MPH vs MSPH vs MHS does push you toward different types of roles.
1. Typical Roles with an MPH
Most MPH grads in the US end up in applied public health practice across government, hospitals, NGOs, and industry. Common job families: (publichealthdegrees.org)
- Public health program manager / coordinator (local/state health departments, NGOs, global health projects)
- Health educator / health promotion specialist
- Community health worker / outreach coordinator (often in more senior/specialist roles if you have an MPH) (Coursera)
- Epidemiology or surveillance officer in health departments (especially with an epi concentration) (graduate.northeastern.edu)
- Health services manager / healthcare administrator (hospitals, clinics, integrated systems) (publichealthdegrees.org)
- Policy analyst / public health consultant in government, nonprofits, or consulting firms (medicine.tufts.edu)
Salary reality:
- Columbia Mailman reported average salary for its MPH grads around $83,800/year (2019–2020 cohort). (Coursera)
- Epidemiologists (where many MPH + epi grads land) have a US median salary around $83,980 according to BLS data summarized by Coursera. (Coursera)
- Community-oriented roles like community health workers sit lower, around $51,000 median, but they’re also not the ceiling for MPH-level work. (Coursera)
- Higher-level positions like public health director can sit in the $150k+ range in some markets. (graduate.northeastern.edu)
MPH doesn’t magically guarantee those numbers, but it gives you the credential and skills to move out of low-skill roles and into mid- to high-level public health positions as you gain experience.
2. Typical Roles with an MSPH
MSPH grads are usually funneled into research and analytics-heavy roles:
- Epidemiologist (surveillance, outbreak investigation, analytic epi, pharmacoepi)
- Biostatistician / data analyst in health systems, research institutes, pharma/biotech (Coursera)
- Public health researcher / research associate in universities, CDC-type institutes, NGOs
- Policy / health services research analyst (think big datasets, regression, “methods” people) (Masters Portal)
MSPH is essentially marketed (accurately) as the degree for people who want research or academic careers. (Masters Portal)
Salary reality (job-family based):
- Epidemiologists: median around $84k, with the top 10% clearing $134k+; those in scientific research settings can have medians around $130k. (Coursera)
- Biostatisticians / statisticians: median salaries over $100k with strong growth prospects. (Coursera)
The MSPH itself isn’t a magic salary booster, but the job types it opens (epi, biostats, research) tend to sit in higher bands than generic outreach roles.
3. Typical Roles with an MHS
MHS is broader as a category, but in the US it usually links to health science / health services / clinical or management tracks: (Nurse.org)
- Healthcare administrator / manager (clinical departments, ambulatory centers, specialty services)
- Clinical research coordinator / clinical trials manager
- Health data analyst / health informatics roles
- Allied health or clinical leadership roles (depending on your original degree – e.g., nurse + MHS)
- Health science educator or academic roles in colleges with a teaching focus
MHS is very program-dependent – one school’s MHS might be health leadership, another’s heavy research, another’s global health. But overall, it plays in the healthcare + public health interface, often pushing you towards management or technical specialist roles. (Bouvé College of Health Sciences)
Salary reality (again, by job family, not letters):
- Master’s in health science can move you into higher-responsibility clinical/management roles, which typically pay more than baseline clinical staff or general admin. (PBA • Palm Beach Atlantic University)
- Roles like healthcare administrator, clinical manager, data analyst commonly land in the $70k–$120k+ range, depending on sector and experience. (Bouvé College of Health Sciences)
If your MHS is in a narrow niche (e.g., clinical research, health informatics), your salary trajectory will follow that industry, not some generic “MHS number.”
4. Hard Truth: Degree Title vs Job Market
A few things you shouldn’t kid yourself about:
- Most US job postings say: “Master’s in public health, epidemiology, biostatistics, health science, or related field.” They don’t say “MPH only” vs “MSPH only” 99% of the time. They care about concentration + skills + experience, not your exact three letters. (publichealthdegrees.org)
- Sector matters more than letters. Federal agencies, big hospitals, pharma, consulting, and tech tend to pay more than tiny NGOs or small local nonprofits – regardless of whether you did MPH or MSPH. (Bureau of Labor Statistics)
- A good CEPH-accredited program + relevant concentration + strong practicum / thesis is worth more than a random non-accredited degree with a fancy label. Some US employers explicitly prefer or require CEPH-accredited programs. (Walden University)
So if you’re obsessing over “which one pays more, MPH or MSPH or MHS,” you’re asking the wrong question. You should be asking:
“Which degree gives me the skills and portfolio to compete for the job family I actually want?”
Common Misconceptions About MPH, MSPH, and MHS (And Why They’re Wrong)
Let’s clean up the nonsense that floats around forums, WhatsApp groups, and random “advice” pages.
Myth 1: “MSPH is higher or more prestigious than MPH”
Reality: MSPH is different in orientation, not “higher level.”
- MSPH is generally more academic/research-focused, with heavier methods and a thesis.
- MPH is generally more practice-focused, with mandatory practicum and applied projects. (Masters Portal)
In US public health practice, MPH is actually the default professional degree employers recognize. MSPH is great if you want research, but it doesn’t sit above MPH in some formal hierarchy.
Myth 2: “MHS is just a weaker or cheaper MPH”
Garbage.
- MHS programs are often highly specialized master’s in health science or specific public health subfields (e.g., clinical research, leadership, health policy, global health). (Nurse.org)
- Some MHS tracks are very rigorous, with strong methods and research expectations; others are built for working professionals who want targeted leadership or clinical skills.
What makes an MHS strong or weak isn’t the label – it’s the school, curriculum, accreditation, and how well it matches your goals.
Myth 3: “MPH can’t lead to research or PhD – you must do MSPH”
No.
- Plenty of epi/biostats PhD and DrPH students start with an MPH, especially if they chose quant-heavy concentrations and did a serious capstone or research project. (graduate.northeastern.edu)
- The real requirement for doctoral programs is evidence of research ability and quantitative competence – which you can absolutely build in an MPH if you’re intentional.
MSPH (or a research MHS) makes the path more straightforward if you want to be a pure methods/data person. But an MPH with strong epi/biostats and published work is still completely valid for PhD entry.
Myth 4: “Any master’s in public health/health science = automatic six-figure salary”
Completely delusional.
- BLS and multiple career sources show wide salary ranges across public health roles:
- Community health and counseling roles sit near $50–60k. (Coursera)
- Mid-level jobs like epidemiologist, environmental scientist, and health services manager often cluster around $80k–100k+. (Coursera)
- Senior leadership (directors, execs, high-level consultants) can reach $150k+, but that’s about experience and responsibility, not “year 1 after the degree.” (graduate.northeastern.edu)
The degree simply moves your ceiling up and gives you entry into professions where high pay is possible – it doesn’t erase the need for experience, performance, and smart career moves.
Myth 5: “The title matters more than accreditation and program quality”
Again, wrong priority.
- CEPH accreditation is a big deal in the US. It’s essentially the quality benchmark for public health programs; some employers and fellowships explicitly prefer or require a CEPH-accredited MPH/MSPH. (Walden University)
- Accreditation affects:
- Whether your training meets recognized competency standards
- Eligibility for things like the CPH exam and some fellowships
- How comfortable employers are trusting your preparation (Ceph)
A mediocre non-accredited MPH/MHS/MSPH with weak practicum/thesis is less useful than a solid CEPH-accredited MPH/MSPH from a program that actually trains you properly.
Myth 6: “Choosing one degree locks you out of all other types of roles”
No, but it tilts the odds.
- An MPH grad with very strong methods, a serious project, and good networking can still get research jobs.
- An MSPH grad who builds leadership and management skills can still move into policy, management, or program leadership roles.
- An MHS grad with strong practice experience can still work in public health programs.
The degree frames your default path. Your experience, network, and side projects decide how far you bend or break that path.
How to Choose the Actual Program (Not Just the Degree Title)
You’re past the “MPH vs MSPH vs MHS” confusion now. Next question is sharper:
“Which specific program in the US should I trust with 2 years of my life and a pile of money?”
Here’s how to choose like an adult, not like someone hypnotized by rankings.
1. Non-Negotiable #1: CEPH Accreditation
If you’re planning to work in public health in the US, this is not optional.
- CEPH (Council on Education for Public Health) is the main accreditor for public health programs in the US. (ceph.org)
- Graduating from a CEPH-accredited program can be required or strongly preferred for:
- US Public Health Service jobs
- Some military public health roles
- Some state and local government agencies and international NGOs (Walden University)
- CEPH accreditation also:
- Sets minimum standards for curriculum & competencies
- Often makes you eligible for the CPH exam, which some employers view as a plus (memphis.edu)
If a program is not CEPH-accredited, you should have a very specific reason for still considering it (e.g., unique niche, country-specific context). Otherwise, skip it.
Use:
- CEPH’s own site to verify accreditation status. (ceph.org)
- Your own site (BestPublicHealth.com) already has a 2025 guide listing CEPH-accredited MPH programs with filters – use that for internal linking and as a resource hub. (bestpublichealth.com)
2. Decide Format First: On-Campus vs Online vs Hybrid
This is logistical but huge.
Key questions:
- Do you need to work while studying?
- Are you okay relocating to the US (visas, cost of living, etc.)?
- Do you want in-person networking, or is online fine?
Major public health orgs (ASPPH, PublicHealth.org, etc.) consistently tell students to decide delivery + location early: on-campus, online, or hybrid. (aspph.org)
Reality:
- Online/hybrid MPH/MSPH can be very good if they’re CEPH-accredited and attach you to real practicum sites.
- Garbage unaccredited “online MPH” programs exist and should be avoided.
So your first filter after accreditation should be:
“Given my life situation, is this full-time in person, part-time online, or hybrid for me?”
3. Read the Curriculum Like a Contract
Most people glance at course titles and then decide based on vibes. That’s stupid.
You should:
- Open the full curriculum page (required + elective courses, credit hours). (Johns Hopkins Public Health)
- Check:
- How many methods courses? (epi, biostats, research design, advanced methods)
- How many practice/management courses? (program planning, management, policy, leadership)
- Any specialization tracks that match your target role (epi, global health, health policy, health economics, etc.)
- Confirm:
- Is there a practicum / applied practice experience?
- Is there a thesis, master’s essay, or just a capstone/project?
Cross-check this with your target:
- You → practice: you want more practicum & management, still some methods, not thesis-obsessed → program should look like a proper MPH. (Upstate Medical University)
- You → research/PhD: you want heavier methods + clear thesis/essay/research project expectations → MSPH or a research-oriented MHS/MS. (U-M School of Public Health)
If the curriculum is 80% fluffy “leadership”, “communication” and “health promotion” with almost no serious epi/biostats, and you say you want a research career—you’re lying to yourself.
4. Look at Admissions Requirements and See If They Respect Standards
Example: Johns Hopkins’ MPH requires:
- Two years of full-time, post-bachelor health-related work experience, or certain doctoral backgrounds. (Johns Hopkins Public Health)
- Prior coursework in math, biology, and a health-related science. (Johns Hopkins Public Health)
This is what a serious program looks like: it demands some baseline competence and experience.
Red flag patterns:
- “No background, no experience, no problem – just pay.”
- Admissions process looks like a factory, not a graduate school (zero mention of faculty, research fit, or competencies).
If the entry bar is ultra-low and the price is high, that’s not “accessibility”, that’s harvesting tuition.
5. Check Outcomes, Not Marketing
Ignore the pretty photos. Look for hard outcomes:
- Employment stats:
- % employed within 6–12 months
- Types of roles (e.g., epi, program management, research, admin)
- Example employers (CDC, state health departments, NGOs, hospitals, consulting) (OMD)
- Further study:
- How many grads go on to PhD/DrPH, MD, or other advanced training? (PMC)
If a program never shows where graduates end up, that’s a data point in itself.
6. Cost, Funding, and Opportunity Cost
Obvious but people still ignore it:
- Compare tuition + fees + living costs between cities/programs.
- Look for:
- Scholarships, assistantships, teaching/research positions
- In-state vs out-of-state tuition differences
- Part-time/online options that let you work concurrently (publichealth.org)
And be honest: An extra $40k in debt isn’t worth it just to put a slightly fancier logo on your CV if the training quality and outcomes are similar.
7. Use Tools That Actually Help (Not Random Blogs)
- ASPPH Academic Program Finder lets you filter by degree type, format, and focus area across member schools. (aspph.org)
- CEPH has directories of accredited schools/programs. (ceph.org)
- Your own site’s CEPH-accredited MPH guide can serve as a curated hub + internal SEO pillar for your article. (bestpublichealth.com)
Use those instead of “some guy in a forum said X is good.”
8. Sanity Check: Fit With Your Life and Personality
Hard reality:
- If you hate statistics, don’t pick a methods-heavy MSPH and then cry later.
- If you hate networking and fieldwork, don’t choose a super practice-heavy MPH and expect to magically enjoy it.
- If you’re already overloaded with life, picking a full-time, in-person, intensive program in an expensive US city is a good way to burn out.
The program has to match who you are now and who you want to become, not who you’re pretending to be for LinkedIn.
Final Verdict & Fast Checklist (So You Actually Decide)
Time to compress the entire article into a decision framework you can’t hide from.

1. Brutal Degree Mapping: MPH vs MSPH vs MHS
If you strip everything down:
- MPH
- Best for: Public health practice, programs, policy implementation, NGO/government work
- Signature: broad public health core + practicum/capstone
- Typical endgame: health departments, NGOs, hospitals, global health projects, mid–senior program roles (Upstate Medical University)
- MSPH
- Best for: Research, data-heavy roles, PhD/DrPH track
- Signature: heavier methods (epi/biostats) + thesis/master’s essay + often field placement
- Typical endgame: epidemiologist, biostatistician, research scientist, academic pathway (U-M School of Public Health)
- MHS
- Best for: Niche specialization in a defined area, either research or targeted practice
- Signature: program-dependent; focused curriculum in one domain (e.g., health leadership, clinical research, global health, health science)
- Typical endgame: specialized technical or leadership roles depending on track and prior background (blog.jmir.org)
2. 10-Point Checklist (If You Can’t Say “Yes” to Most of These, Don’t Apply)
For each program you’re considering, ask:
- Is it CEPH-accredited?
- Does the degree type match what I actually want to do (practice vs research vs niche)?
- Do the required courses match the skills I want? (not just the marketing slogans)
- Is there a practicum or thesis structure aligned with my goal?
- Are admissions requirements serious enough to indicate they’re selective (not just “pay & join”)? (Johns Hopkins Public Health)
- Do they publish real outcome data (jobs, employers, further study)?
- Is the cost sane* relative to expected salary + my financial situation?
- Is the format realistic for my life (online vs in-person, full- vs part-time)? (publichealth.org)
- Are there faculty / research groups / practice partners that clearly match my interests? (blog.jmir.org)
- Would I still choose this program if I had to remove the brand name from my CV?
- If the answer is “no” and you’re only going for prestige, that’s a red flag.
3. If You’re Still Stuck, Ask This One Question
Forget everything else and answer:
“In 5–7 years, do I want people to see me primarily as a public health practitioner, a researcher, or a specialist in a very specific area?”
- Practitioner → MPH
- Researcher / PhD/DrPH → MSPH (or research-heavy MHS/MS)
- Niche specialist → MHS (or a tightly focused MSPH/MPH concentration that matches that niche)
If your answer changes every time you think about it, your problem isn’t the degree—it’s that you haven’t decided who you want to be. The degree won’t fix that confusion; it will just make it more expensive.
FAQ – Fast Answers to the Questions Everyone Keeps Asking
1. Is MSPH better than MPH?
No – it’s different, not “higher.”
- MPH is usually the standard professional practice degree in public health – built for people who want to work in health departments, NGOs, hospitals, and programs.
- MSPH is usually the research-heavy public health science degree – built for people who want stronger methods and a clearer path to research or PhD work.
Employers in public health practice often treat the MPH as the default credential; research groups and PhD committees may look more closely at MSPH or at how research-heavy your MPH/MHS was. The value comes from skills + thesis/practicum + school quality, not the letters alone.
2. Is MHS equivalent to an MPH?
Usually not.
- An MPH is designed as a broad public health practice degree with core public health domains and mandatory applied training (practicum/capstone).
- An MHS (or MHSc) is a specialized health science degree, often narrower in focus and highly dependent on the department and school.
Some MHS programs are very close to a research-oriented public health degree; others focus more on health leadership, clinical research, or a specific niche. You cannot assume “MHS = MPH” without reading the exact curriculum and outcomes for that specific program.
3. Which degree is best for epidemiology – MPH, MSPH, or MHS?
If your priority is epidemiology as a career or PhD epi later:
- Choose an MSPH in Epidemiology or an MHS/MS in Epidemiology if you want maximum methods depth and a thesis.
- Choose an MPH with an Epidemiology concentration if you want a balance of epi + broader public health practice (good if you want field epi, surveillance, outbreak work, etc., not just academic epi).
Your decision should be based on:
- How much statistics/methods you actually want,
- Whether you want a thesis, and
- Whether your endgame is practice epi in health departments vs research epi / PhD.
4. Can an MPH still lead to a PhD or research career?
Yes, absolutely – if you use it properly.
An MPH can lead to a PhD/DrPH if:
- You take quantitatively demanding courses (epi, biostats, methods) instead of hiding in only soft electives.
- You do a serious capstone/research project, ideally with real data and a supervisor who can write a strong reference.
- You get research experience (assistantships, projects, publications) while studying.
An MSPH or research MHS just makes the “research” signal louder by default, but a strong MPH is still a perfectly valid route into doctoral programs.
5. Which degree has the highest salary potential: MPH, MSPH, or MHS?
None of them magically guarantees a specific salary. What matters is:
- Job family (epi, biostats, health services management, consulting, clinical research, NGO program work, etc.)
- Sector (federal/state government, hospitals, pharma, consulting, NGOs, academia)
- Experience and responsibility level
Rough pattern:
- Research/data roles common after MSPH or quant-heavy MPH/MHS (epi, biostats, health data science) often sit in higher bands than entry-level community roles.
- Leadership/management roles (health services manager, program director) can also climb high over time, regardless of whether you did MPH, MSPH, or MHS.
So the smarter question is:
“Which degree gets me into the type of role and sector that typically pays what I want?”
6. Do employers in the US really care about CEPH accreditation?
Many do – and you should.
- CEPH accreditation is the main US quality benchmark for public health programs.
- Some employers, fellowships, and government roles explicitly prefer or require a degree from a CEPH-accredited school or program.
- It also ties into eligibility for certifications like the Certified in Public Health (CPH) exam.
If you’re choosing between similar programs and only one is CEPH-accredited, the accredited one is usually the safer long-term bet.
7. Can I switch from practice to research (or vice versa) after I pick a degree?
You can, but the further you move from your degree’s “default path,” the more extra work you’ll need:
- MPH → research/PhD: you’ll need to deliberately load up on methods, pursue research projects, and maybe do extra coursework or certificates.
- MSPH/MHS → practice/leadership: you’ll need to build experience running programs, leading teams, and working with real systems, not just doing analysis.
The degree sets your starting direction, not an unbreakable prison. Your choices during and after the degree (jobs, projects, networks) are what actually decide where you end up.
8. What’s the single biggest mistake people make when choosing between MPH, MSPH, and MHS?
They obsess over the label and ignore:
- The actual curriculum,
- The quality and accreditation of the program,
- The type of work graduates actually end up doing, and
- Their own personality and long-term goal.
If you pick a research-heavy MSPH but you hate stats, or a practicum-heavy MPH but you hate fieldwork, that’s not a “degree problem” – that’s you not being honest with yourself.
Internal Links:
CEPH-Accredited MPH Programs in New York (2025)
Accelerated 1-Year MPH Programs (2025 Guide): Accredited 12-Month MPH Options
MPH vs MHA vs MBA (2025): Which Health Degree Is Best for You?
Related MPH Guides
Use these linked guides to compare degree fit, accreditation, and costs before you apply.
MPH vs MSc Public Health (UK & International Degrees)
The difference between an MPH and an MSc in Public Health is mostly geography and emphasis. The MPH is the standard professional public health degree in the United States (and widely offered globally), built around applied practice—practicum hours, a capstone, and CEPH accreditation. The MSc Public Health is the common format in the UK, Europe, and many Commonwealth countries (e.g., LSHTM, Imperial College): typically a one-year, research-leaning degree with a dissertation instead of a practicum.
- Recognition: U.S. employers and government roles generally expect the MPH (ideally CEPH-accredited). UK/international employers treat the MSc Public Health as the equivalent professional credential.
- Structure: MPH = coursework + applied practicum + capstone (usually 42–48 U.S. credits, 1–2 years). MSc = coursework + research dissertation (usually 12 months full-time in the UK).
- Moving between systems: A UK MSc in Public Health is normally accepted for U.S. PhD/DrPH admission and most private-sector roles, but some U.S. government positions specify a CEPH-accredited degree—check the job series requirements before choosing.
- MS/MSc vs MSPH: A U.S. MS in public health fields and the MSPH both lean research/thesis; the MSc is simply the international naming of the same research-first idea.
Is an MSc Public Health equal to an MPH?
Functionally yes for most careers: both are master’s-level public health credentials. Choose the MPH if you’ll work in the U.S. system (especially government/health-department roles that reference CEPH accreditation); choose the MSc if you’ll work in the UK/EU/international system or want a faster, research-oriented route into a PhD.
Difference between an MS and an MPH, in one line
The MPH trains you to practice public health (programs, policy, field epidemiology); an MS/MSc/MSPH trains you to research it (methods depth, thesis, PhD pipeline). Pick by destination, not by name.
