
Choosing between MPH vs MHA vs MBA can feel impossible when every brochure promises “leadership in healthcare.” This guide cuts through the noise and shows, in plain language, what each degree actually teaches you, the jobs it leads to, and how to pick the one that matches your real career goals.
Table of Contents
MPH vs MHA vs MBA at a Glance (Quick Answer & Comparison Table)
If you strip away all the marketing language, the difference is simple:
- An MPH is about population health, prevention, and policy.
- An MHA is about running hospitals and health systems.
- An MBA (with healthcare focus) is about business and management skills you can use in or outside healthcare.
In practice:
- Choose an MPH if you care about communities, data, disease patterns, and health equity.
- Choose an MHA if you want to manage hospitals, clinics, or health systems and own the operations, budgets, and teams.
- Choose an MBA if you want maximum flexibility across industries (consulting, tech, finance, healthtech) and are okay with healthcare just being one possible niche.
Quick Comparison Table
| Degree | Primary Focus | Typical Students / Background | Common Jobs | Typical US Salary Range* | Can Work Outside Healthcare? |
|---|---|---|---|---|---|
| MPH (Master of Public Health) | Population health, prevention, epidemiology, biostatistics, policy, social determinants of health | Public health officers, nurses, doctors, NGO workers, social science grads, people already in government or community programs | Epidemiologist, public health analyst, program manager, health educator, policy analyst | Roughly mid-$60K to low-$100K+ depending on role, location, and experience | Yes, but mainly in health-adjacent roles (NGOs, government, research, global health, some private sector) |
| MHA (Master of Health Administration) | Health-care delivery systems, hospital operations, finance, strategy, quality improvement, HR | People who want to manage hospitals/clinics, early-career administrators, some clinicians moving into leadership | Hospital/clinic administrator, health services manager, operations manager, practice manager, quality improvement manager | Commonly high-$70K to $120K+; senior leaders and executives can go well above that | Mostly tied to healthcare and health services organizations |
| MBA (Healthcare Focus or with Health Electives) | General business: finance, accounting, strategy, marketing, operations, leadership, plus optional healthcare electives | Business, engineering, economics, or science graduates; consultants; people pivoting into healthtech, pharma, or broader business leadership | Management consultant, strategy manager, product manager (healthtech/pharma), operations director, general manager | Often starts in the $80K–$120K+ range; top programs and consulting/tech roles can go significantly higher | Yes, very – can work in any industry, not just healthcare |
*Salary ranges are broad estimates meant for comparison, not guarantees. Sector (public vs private), country, city, and your prior experience can easily move you above or below these bands.
What Each Degree Actually Focuses On
Understanding the core focus of each degree is more important than obsessing over the letters. The curriculum tells you what problems the degree trains you to solve.
MPH – Master of Public Health
An MPH trains you to think in terms of populations, not single patients. You are not asking “How do I treat this one person?” but “Why is this disease happening here, in this group, right now – and how do we stop it at scale?”
Typical emphasis areas include:
- Epidemiology – studying patterns and causes of disease in populations, designing studies, and interpreting data.
- Biostatistics – turning messy health data into evidence you can actually act on.
- Health policy and management – how laws, regulations, health systems, and financing models shape who gets care and who doesn’t.
- Social and behavioral sciences – how behavior, culture, income, education, and environment drive health outcomes.
- Environmental and occupational health – air, water, food, workplaces, and climate as determinants of health.
Typical students:
- Public health officers, NGO staff, nurses, junior doctors, social science grads, and people already working in government programs or community projects.
Typical settings after graduation:
- Government health departments, NGOs, international agencies, research institutes, universities, and large public-health programs (immunization, TB/HIV, maternal and child health, NCD prevention, etc.).
If you enjoy data, policy, community work, and prevention, the MPH is aligned with how you naturally think.
MHA – Master of Health Administration
An MHA is the degree for people who want to run the system: hospitals, clinics, health systems, managed-care organizations, or large health service networks.
Instead of asking “How do we reduce diabetes in this district?”, you are asking “How do we make this hospital work better – financially, operationally, and clinically – for the people it serves?”
Core focus areas typically include:
- Healthcare operations and logistics – patient flow, bed management, scheduling, throughput, and process redesign.
- Healthcare finance – budgets, reimbursement models, revenue cycle, cost control, and financial sustainability of hospitals/health systems.
- Strategy and quality improvement – strategic planning, accreditation, quality metrics, patient safety, and performance dashboards.
- Human resources and leadership – staffing, labor relations, team leadership, change management.
- Health-care law, ethics, and regulation – compliance with government rules, insurance regulations, and accreditation standards.
Typical students:
- People already in hospital administration, clinic managers, mid-level coordinators, or clinicians (doctors, nurses, pharmacists, dentists) who want to move into management and leadership instead of full-time clinical work.
Typical settings after graduation:
- Hospitals, health systems, outpatient networks, specialty clinics, insurance organizations, and sometimes consulting firms that work primarily with health providers.
If you want decision-making power inside hospitals – budgets, staffing, policies – MHA is the direct path.
MBA – Master of Business Administration (with Healthcare Focus)
An MBA is fundamentally a business degree, not a health degree. You are trained to run or advise organizations in any industry: health, tech, banking, manufacturing, NGOs, whatever. A healthcare-focused MBA simply lets you apply those skills to healthcare if you want.
The core of the degree usually covers:
- Finance and accounting – understanding financial statements, investments, valuation, and budgeting.
- Strategy – how organizations compete, grow, and position themselves in markets.
- Marketing and customer insights – understanding users/patients/customers and designing services around them.
- Operations and supply chain – how products and services are delivered efficiently and reliably.
- Leadership and organizational behavior – managing teams, culture, and change.
Then, on top of this, you can add:
- Healthcare electives – like health economics, healthcare strategy, pharma management, healthtech product management, payer-provider dynamics, etc.
Typical students:
- Business, engineering, or science grads; consultants; analysts; people wanting to pivot into healthtech, pharma, insurance, consulting, or general management.
Typical settings after graduation:
- Consulting firms, healthtech startups, pharma and med-device companies, insurers, hospital corporate offices, and also non-health sectors (tech, finance, consumer goods, etc.).
If you want maximum flexibility, care a lot about business and strategy, and you are okay with healthcare being just one of several options, an MBA is usually the better fit than a pure health degree.
Who Should Choose MPH, MHA, or MBA? (Profiles & Goals)
Forget the abstract marketing language and match who you are + what you actually want to do to each degree.
I’m going to be blunt: if you can’t tie the degree to specific job titles and work settings, you’re just buying an expensive identity badge.
1. You Want Public Health Programs, Policy, or Global Health → MPH
You’re a fit for an MPH if most of this sounds like you:
- You think in terms of communities and populations, not just individual patients.
- You care about prevention, social determinants of health, and health equity.
- You like data, surveys, research, and field work more than spreadsheets full of hospital revenue.
- Ideal problems you want to work on:
- “How do we reduce maternal mortality in this province?”
- “How do we design a vaccination campaign that actually reaches high-risk groups?”
- “How should we update this national guideline to be realistic for low-resource settings?”
Best-fit roles after an MPH:
- Epidemiologist or surveillance officer
- Public health analyst / health data analyst
- Program manager (HIV, TB, NCDs, RMNCH, mental health, etc.)
- Health promotion / health education specialist
- Policy analyst in government, NGOs, or global-health agencies
In the US, roles like epidemiologist and biostatistician are projected to grow far faster than average (around 16–27% growth from 2024/2025 into the 2030s, depending on the specific occupation and time window), reflecting long-term demand for people who can interpret health data and inform policy. (Bureau of Labor Statistics)
Choose MPH if:
- You want to work in ministries of health, WHO/UN agencies, NGOs, research centers, or academic public health.
- You’re okay with salaries that grow steadily but are usually lower than top corporate/consulting tracks, especially early on.
- You care about impact on populations more than maximizing corporate pay.
2. You Want to Run Hospitals or Health Systems → MHA
You’re a fit for an MHA if this sounds closer to you:
- You like systems and operations: how a hospital runs day to day.
- You’re comfortable with budgets, staffing, and process redesign.
- You want to be on the management side of healthcare, not just a clinical or field worker.
- Ideal problems you want to work on:
- “How do we reduce emergency department waiting times by 30%?”
- “Why is this ward overstaffed while another is collapsing under workload?”
- “How do we keep the hospital financially alive without compromising quality?”
Best-fit roles after an MHA:
- Hospital or clinic administrator
- Medical and health services manager
- Operations director / service line manager
- Quality improvement manager / patient safety lead
- Practice manager for multi-specialty or primary-care networks
In the US, medical and health services managers are projected to grow by about 23% from 2024–2034, far above the average for all occupations – one of the strongest management job outlooks in any sector. (Bureau of Labor Statistics)
Choose MHA if:
- You want to live inside hospitals, clinics, health systems, or insurers, not general corporations.
- You’re willing to own hard operational decisions: hiring/firing, budgeting, dealing with complaints and regulators.
- You want income and responsibility that scale with leadership roles inside provider organizations.
If the idea of dealing with beds, budgets, and bureaucracies bores you, don’t do an MHA. You will hate your work.
3. You Want Broad Business Options In and Beyond Healthcare → MBA (with Healthcare Focus)
You’re a fit for an MBA if:
- You’re more excited by strategy, product, markets, and business models than by government programs or hospital wards.
- You want the option to work in healthtech, pharma, consulting, insurance, or even outside healthcare entirely.
- Ideal problems you want to work on:
- “How do we scale this digital health product to 1 million users?”
- “How do we redesign this insurance benefit so it’s profitable and still attractive?”
- “How do we help a hospital group cut costs by 15% without destroying quality?”
Best-fit roles after an MBA (healthcare focus):
- Management consultant (healthcare or generalist)
- Product manager or strategy manager in healthtech / telehealth / med-tech / pharma
- Operations or general manager at a large healthcare company
- Corporate development / business development in health-related firms
- And completely non-health roles in tech, finance, or other sectors
Management analyst/consultant roles are projected to grow around 9–10% between 2022–2032/2024–2034, faster than the overall job market, driven by demand for data-driven efficiency and cost control. (Bureau of Labor Statistics)
Choose MBA if:
- You want maximum flexibility and might leave healthcare later.
- You’re aiming for corporate leadership, consulting, or product/strategy rather than pure public-sector or hospital roles.
- You care a lot about compensation upside and are comfortable competing in a more aggressive business environment.
If you hate the idea of networking, ambiguity, and competition, you may struggle in many MBA-driven career paths.
4. Special Note: Clinicians (Doctors, Nurses, Dentists, Pharmacists)
Clinicians are the ones who usually get stuck and waste years on the wrong degree because of vague goals.
Here’s a harsh but useful way to look at it:
- Clinician + MPH
- Good if you want to leave routine clinical work and move into public health programs, research, policy, or global health.
- Logical for those aiming to work in UN agencies, NGOs, national programs, academic public health.
- Weak choice if your real dream is hospital CEO or corporate leadership – in that case MPH alone is usually not enough.
- Clinician + MHA
- Best if you want to stay within the provider world but move from bedside to management and leadership.
- You’re aiming at roles like medical superintendent, service line leader, hospital director.
- Strong path if you have existing clinical credibility and want to convert that into operational authority.
- Clinician + MBA (sometimes with a health or tech focus)
- Best if you want career flexibility and money – healthtech founder, pharma/med-tech leadership, consulting, insurance, etc.
- Good for people who are done with traditional hospital politics and want to move into innovation, startups, corporate, or consulting.
- Requires you to be okay with stepping out of traditional medical hierarchies and competing head-to-head with non-clinical MBAs.
If you’re a clinician and can’t clearly name at least 2–3 job titles you want after graduation, you’re not ready to pick a degree. Decide roles first, degree second – not the other way around.
Curriculum and Skills Comparison (MPH vs MHA vs MBA)
At this point, you should be asking: “What will I actually learn and be able to do after each degree?”
Let’s break it down at the level of courses, practical work, and skills you’ll walk away with.
1. Core Courses by Degree – What You’ll See on the Transcript
Typical MPH Core – What You Actually Study
An MPH is built around population health and data, not hospital revenue or corporate profit. Most programs follow the same spine, even if course titles change:
- Epidemiology – usually an intro plus a more advanced course; how to study who gets sick, when, where, and why.
- Biostatistics – turning messy health data into usable evidence, often using tools like R, Stata, SAS, SPSS, or similar.
- Public health surveillance and study design – how to track diseases and build studies that actually answer useful questions.
- Health behavior and social determinants – how income, education, gender, culture, and environment shape risk and outcomes.
- Environmental and occupational health – air, water, food, workplaces, and climate as drivers of illness and injury.
- Health policy and health systems – how laws, financing, insurance, and governance determine who gets care and who doesn’t; often with a dose of health economics.
- Research methods and a final project – a capstone, dissertation, or culminating project where you apply all of this to a real public-health problem.
This isn’t just “more theory after undergrad.” A proper MPH is supposed to give you enough tools to move from “I think this is a problem” to “I can prove it, design an intervention, and measure whether it worked.”
What an MPH Actually Equips You to Do
By the time you finish, you should be able to do more than repeat definitions of incidence and prevalence. In real terms, you’ll be able to:
- Design and critique studies – both observational (cohort, case–control, cross-sectional) and intervention trials – and spot weak methods before they waste time and money.
- Work with data instead of guessing – analyze datasets, interpret relative risks and odds ratios, deal with confounding and bias, and translate output into clear conclusions.
- Write policy briefs and recommendations that use evidence, not opinions, to argue for guideline changes, new programs, or revised priorities.
- Plan, implement, and evaluate health programs at community, district, or national level – with clear objectives, indicators, baselines, and follow-up measures.
In short: an MPH trains you to think like someone responsible for population-level decisions, not just individual patient encounters.
You come out able to:
- Read and manage department and hospital-level budgets.
- Model staffing, throughput, and capacity (beds, clinics, theatres).
- Run or support quality improvement projects with measurable outcomes.
- Navigate accreditation, licensing, and regulatory requirements.
- Lead teams and manage conflict in a healthcare environment.
What an MHA Actually Trains You to Do
By the end of a solid MHA, you should be able to do much more than quote buzzwords in meetings. In practical terms, you’ll be able to:
- Make sense of a department’s budget and help plan how money is allocated across a whole hospital or clinic network.
- Work out how many people, beds, and clinic slots you really need instead of guessing or copying last year’s rota.
- Take a messy problem (long waiting times, frequent complaints, low staff morale), design a quality-improvement project, and prove whether it worked with real numbers.
- Prepare your organization for accreditation visits, licensing checks, and regulatory audits without everyone panicking the week before.
- Run meetings, handle difficult staff conversations, and lead teams through conflict and change instead of just forwarding emails.
This is the degree that turns you from “person who complains about the system” into “person who is responsible for fixing it.”
Typical MBA (Healthcare Focus) – What’s Really on the Menu?
An MBA with a healthcare angle is still an MBA first, health second. You’re being trained as a business generalist who can work in healthcare, not a narrow policy specialist.
Most programs start with core business subjects like:
- Financial accounting and corporate finance
- Strategy and competitive positioning
- Marketing, branding, and consumer insight
- Operations and supply-chain management
- Organizational behavior and leadership
- Data analytics and managerial decision-making
Once that foundation is in place, you bolt on healthcare-focused modules, for example:
- Healthcare strategy and innovation
- Health economics and how payers and providers interact
- Management of pharma, med-tech, or biotech companies
- Digital health, telemedicine, and healthtech product management
After a decent MBA you should be comfortable to:
- Break down financial statements and see exactly where a business is leaking or making money.
- Build business cases, pricing strategies, and market-entry plans that hold up under scrutiny from senior leadership or investors.
- Work with designers, engineers, clinicians, and sales teams to launch and scale products or services, including digital health tools.
- Operate naturally inside cross-functional corporate teams, not just within a health department or hospital ward.
If you picture yourself talking about market share, user growth, and unit economics as often as you talk about patients, this is your lane.
2. How Each Degree Lets You Practice in the Real World
Every prospectus promises “applied learning.” The reality is that MPH, MHA, and MBA programs throw you into very different kinds of “real world.”
MPH: On the Ground With Programs and Data
With an MPH, the practical work is usually tied to populations, programs, and evidence:
- A field placement or practicum in a health department, NGO, research project, or global-health initiative.
- A capstone, project, or thesis that uses real data from surveillance systems, surveys, or program dashboards.
- Hands-on work in survey design, data collection, monitoring and evaluation (M&E) and sometimes writing policy notes.
You come out with experience you can point to: “I helped design, run, or evaluate this specific public-health program in this setting.”
MHA: Inside the Hospital Machine
MHA programs are most useful when they push you directly into hospital or health-system operations:
- Administrative residencies or fellowships where you sit in management meetings, not just classrooms.
- Project work focused on operations, finance, or quality, using real hospital data, real staff, and real constraints.
- Close contact with department managers, service-line leaders, and sometimes the C-suite, where you see how decisions are actually made.
Instead of just saying “hospitals should be more efficient,” you learn what happens when you change bed allocation, clinic timing, or staffing on a real ward.
MBA: Internships, Clients, and Case Rooms
MBA “real-world” training is built around employers and markets:
- Summer internships at consulting firms, tech companies, pharma, insurers, or the corporate office of a hospital chain.
- Client projects where your team works on a real problem for a company – which might be a health system, but could just as easily be a bank or a tech startup.
- Case competitions and hackathons, often sponsored by big names in digital health, insurance, or biotech.
If you care about having recognizable brands on your CV and learning how different industries think about problems, this setup is extremely valuable.
3. How “Quant” and Leadership Really Show Up in Each Degree
All three paths involve numbers and leadership, but the flavour is different enough that the wrong match will make you miserable.
MPH: Numbers for Public-Health Decisions
- Heavy emphasis on biostatistics, epidemiology, and research methods.
- You’re handling health and survey data, not profit-and-loss statements.
- You’ll likely use tools like R, Stata, SAS, SPSS, or Python to run regressions, survival analyses, and other models.
Perfect if you enjoy digging into data and evidence, writing up findings, and explaining what the numbers mean for policy or program choices.
Not ideal if you hate statistics or never want to look at a code window in your life.
MHA: Operational Metrics and Managerial Numbers
- Moderate level of quant in healthcare finance, budgeting, and basic analytics.
- Constant attention to operations metrics: occupancy rates, patient flow, length of stay, readmissions, cost per case, etc.
- Leadership training is built around real people and real services – scheduling, performance reviews, morale, and change management.
Good fit if you’re okay with spreadsheets, but your main interest is making services run better and leading teams, not building complex statistical models or investment portfolios.
MBA: Finance Math Plus High-Pressure Leadership
- Finance, accounting, and analytics courses can be mathematically demanding, especially in stronger programs.
- You’ll learn to do NPV, IRR, valuation, market sizing, pricing, and other tools that show up in consulting and corporate strategy.
- Leadership isn’t just a theory class – it’s tested in group work, club roles, recruiting pressure, and networking, often all at once.
This path suits people who are willing to live with competition, ambiguity, and constant judgment from peers, recruiters, and sometimes alumni. If that sounds exhausting rather than exciting, think carefully.
4. The Hidden Curriculum: Soft Skills and Networks
The part almost nobody reads in the brochure – but which actually shapes your career – is the mix of soft skills and networks you build.
MPH: Public-Health and Policy Circles
- Your strongest connections will be in health departments, NGOs, UN agencies, research units, and universities.
- Fantastic if you want to move between ministries of health, international organizations, and academic projects.
- Less useful if your eventual goal is big consulting or mainstream corporate roles, unless you deliberately build that bridge yourself.
MHA: Provider and Health-System Leadership
- Your classmates and alumni will be scattered across hospitals, clinic groups, integrated health systems, and insurers.
- These contacts matter when you’re trying to move from unit manager → departmental leader → executive roles.
- If you know you want to stay inside the provider world, this network is usually more relevant than a generic business one.
MBA: Cross-Industry Mobility and Brand Power
- MBA cohorts are deliberately mixed: consulting, finance, tech, consumer products, startups – healthcare is just one slice.
- In well-known programs, the alumni network can quietly open doors for decades, in multiple countries and industries.
- That makes an MBA especially powerful if you think you’ll change sectors or countries more than once, or if you want the option to leave healthcare entirely later.
If your plan is to spend your career in public or NGO health systems, a good MPH or MHA is usually enough.
Career Paths and Job Titles After MPH, MHA, and MBA
Reading course lists is useless if you can’t picture the job you’ll actually hold. So let’s anchor each degree to real roles people end up in.
After an MPH: Public Health, Programs, Data, and Policy
Most MPH graduates end up in roles that sit between the community and the system – not in a clinic, not in a boardroom, but in the engine room of public health.
Typical MPH-type roles (titles obviously vary by country):
- Epidemiologist / Surveillance Officer – tracking outbreaks, analyzing trends, advising on control measures.(Bureau of Labor Statistics)
- Public Health / Health Data Analyst – cleaning and analyzing datasets, producing dashboards, advising decision-makers.
- Program Manager / Coordinator for TB, HIV, NCDs, maternal and child health, mental health, etc.
- Health Education Specialist / Health Promotion Officer – designing campaigns, community sessions, social media health content.(Bureau of Labor Statistics)
- Monitoring & Evaluation (M&E) Specialist – designing indicators, logframes, and evaluation plans for projects.
- Policy Officer / Policy Analyst in a ministry of health, WHO office, UN agency, or NGO.
Where they usually work:
- Ministries / Departments of Health
- National disease control programs
- UN agencies (WHO, UNICEF, UNFPA, etc.) and other multilaterals
- International and local NGOs
- Universities, research institutes, and think tanks
If you want to argue for or design a vaccination campaign, mental health program, or national screening guideline, this is the lane.
After an MHA: Hospital and Health-System Leadership
MHA graduates live inside provider organizations – the places that actually deliver care: hospitals, clinic chains, integrated health systems, sometimes insurers.
Common MHA-type roles:
- Medical and Health Services Manager / Hospital Administrator – running departments, clinics, or whole facilities.(Bureau of Labor Statistics)
- Operations Manager / Service Line Director – responsible for a particular area (surgery, emergency, oncology, primary care, etc.).
- Quality Improvement / Patient Safety Manager – leading projects on waiting times, infection control, readmissions, safety culture.
- Practice Manager – managing multi-physician clinics, outpatient centers, diagnostic centers.
- Project Manager (Hospital Transformation / EHR / Accreditation) – coordinating big change projects and keeping departments aligned.
Typical employers:
- Public and private hospitals
- Clinic networks and ambulatory care centers
- Integrated delivery systems and HMOs
- Health insurance companies and third-party administrators
- Large specialty practices and diagnostic chains
If you want responsibility for beds, staff, budgets, metrics, and patient flow, an MHA is designed for that world.
After an MBA (Healthcare Focus): Strategy, Product, and Corporate Roles
MBA graduates with a healthcare focus don’t usually become “public health officers” or “ward managers.” They go where money, strategy, and products live.
Healthcare-related roles:
- Management Consultant (healthcare practice or generalist) – advising hospitals, insurers, pharma, or healthtech companies on strategy and operations.(Bureau of Labor Statistics)
- Product Manager / Product Lead in digital health, SaaS, med-tech, or insurance.
- Strategy Manager / Corporate Development in hospital groups, insurers, pharma, or med-tech firms.
- Operations / General Manager for healthtech startups, telemedicine platforms, or service lines inside larger companies.
Non-health roles that are still realistic after the same degree:
- Consultant in non-health sectors (energy, banking, public sector, tech).
- Roles in big tech, fintech, consumer products, or logistics.
- Founding or scaling a startup (health or non-health).
If your dream day involves board slides, market analysis, and product roadmaps, not field visits or ward rounds, this is the ecosystem you’re optimizing for.
Red-Flag Check
If you read all three lists and none of the roles sound like something you’d be proud to put on a nameplate, your problem is not “Which degree?” – it’s “What do I actually want my workday to look like?” Don’t hide that confusion under a new three-letter acronym.
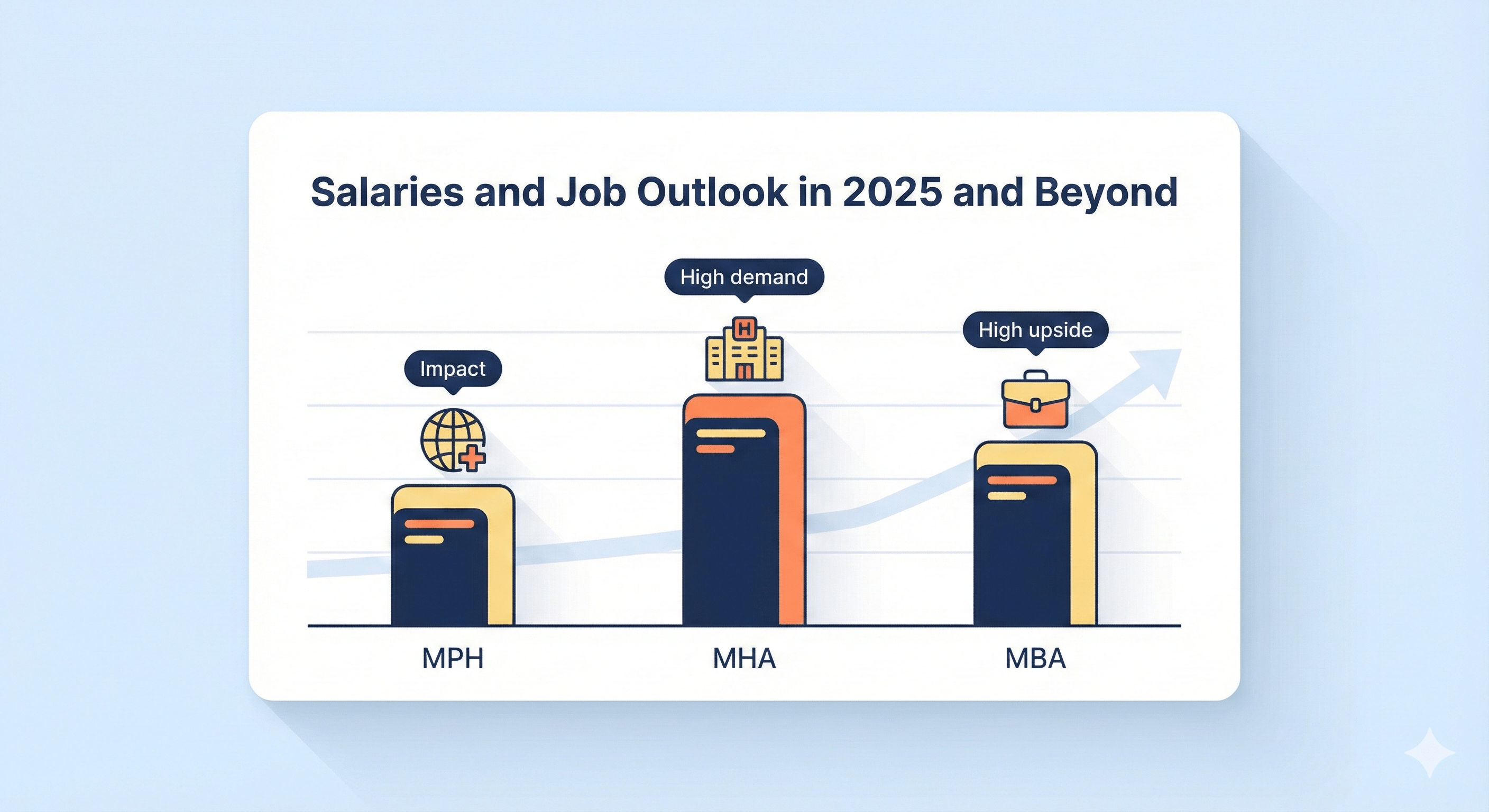
Salaries and Job Outlook in 2025 and Beyond
Now the part everyone pretends not to care about: pay and demand.
I’ll use recent U.S. data (because it’s transparent and updated), mainly from the Bureau of Labor Statistics. Numbers will be different in Pakistan, the UK, Gulf, etc., but the relative pattern between MPH vs MHA vs MBA roles is similar: management and consulting usually pay more than pure public-sector roles; demand for health-related roles is strong almost everywhere.
MPH-Style Roles: Decent Pay, Strong Social Impact, Moderate Ceiling
Representative U.S. roles and numbers:
- Epidemiologists
- Median pay around $83,980/year (May 2024).
- Projected growth about 16% from 2024–2034, much faster than average. (Bureau of Labor Statistics)
- Health Education Specialists
- Median pay roughly $63,000/year (May 2024). (Bureau of Labor Statistics)
- Community Health Workers
- Median pay about $51,030/year (May 2024).
- Projected growth around 11% from 2024–2034, also faster than average. (Bureau of Labor Statistics)
Program managers and M&E specialists in big NGOs or UN projects often sit above these medians, especially with experience and international postings, but those roles are more variable and strongly depend on employer and country.
What this means in plain terms:
- You’re unlikely to be rich, but you can reach a comfortable middle-class income in high-income countries and a solid professional income in LMIC settings.
- Demand is structurally strong – aging populations, NCDs, climate change, pandemics – all push more funding into public health.
- The real trade-off is pay vs. impact vs. bureaucracy. Public health can be fulfilling but often slow, political, and grant-dependent.
MHA-Style Roles: High Demand, Strong Management Pay
Here the numbers jump.
- Medical and Health Services Managers (this category includes hospital administrators, clinic managers, etc.):
- Median pay around $117,960/year (May 2024).
- Projected growth around 23% from 2024–2034, far above the average for all occupations. (Bureau of Labor Statistics)
In other words:
- This is one of the fastest-growing management careers anywhere in the economy.
- Pay scales very well with responsibility – department managers, service-line directors, and C-suite executives can go well above the median, especially in large systems or private networks.
- On the flip side, these roles come with constant pressure: regulatory changes, staffing shortages, angry patients, unhappy clinicians, and financial constraints, often all at once.
In the Gulf, UK private sector, and many middle-income countries, strong MHA-type profiles can do very well financially, but the spread is huge – public hospitals pay less; private hospital chains and insurers pay more.
MBA (Healthcare Focus): Broadest Ceiling, Most Competition
MBA outcomes vary the most because you can land in healthcare consulting, general consulting, tech, finance, or corporate roles.
Representative U.S. benchmark:
- Management Analysts / Consultants
- Median pay around $101,190/year (May 2024).
- Projected growth roughly 9% from 2024–2034, faster than average. (Bureau of Labor Statistics)
In reality:
- Top consulting firms, big tech companies, and high-margin healthtech or SaaS businesses can pay well above those medians once you factor in bonuses, stock, etc.
- Lower-tier consulting, small companies, or non-profit roles may sit closer to, or even below, the medians.
- The distribution is wide: some MBAs end up in very ordinary roles with only slightly higher pay than MPH/MHA paths, especially if the school brand is weak or networking is poor.
So you’re trading:
- Higher potential upside (especially if you hit consulting/tech/leadership)
vs - Higher risk and competition (no guaranteed landing, brutal recruiting for top roles, and a big opportunity cost if you choose a mediocre program).
Outside the U.S. – How to Think About It
If you’re in Pakistan, India, the Middle East, or similar contexts:
- Absolute pay numbers are lower, but the hierarchy is similar:
- Hospital management and corporate roles (MHA/MBA-type) usually pay more than most government/NGO public-health roles (MPH-type).
- International NGOs, UN agencies, and donor-funded projects can pay far above local government rates, especially for technical MPH profiles.
- The real value of the degree is often:
- Mobility (can you move country or sector?).
- Signal (does this degree from this school actually impress the employers you care about?).
- Network (who can pick up the phone for you?).
blunt conclusion on money
- If maximum salary and corporate doors are your top priority, and you can get into a strong MBA program, that path usually wins long-term.
- If you want stable, well-paid management roles in healthcare and are sure you’ll stay in hospitals or providers, MHA is a very rational bet.
- If you care most about public health impact, policy, research, and programs, accept that the pay curve is flatter and go MPH, but be intentional about targeting better-paying employers (UN, major INGOs, strong research centers) instead of drifting into the lowest-paid jobs by default.
How to Decide Between an MPH, MHA, and MBA (Without Lying to Yourself)
If you’re still unsure which way to go, it’s probably because you’re treating the degree as the goal. It isn’t. The job you want and the life you want are the goal. The degree is just one tool.
Forget the brochures for a moment and walk through this in order.
1. Start With Job Titles, Not Degrees
Before you even say “MPH vs MHA vs MBA”, answer this:
“If I had to start work six months from now, what 2–3 job titles would I be happy to sign under my email?”
Examples:
- Epidemiologist, Public Health Analyst, Monitoring & Evaluation Officer
- Hospital Operations Manager, Quality Manager, Clinic Administrator
- Product Manager (Digital Health), Strategy Manager, Healthcare Consultant
If you can’t name at least two realistic roles, you’re not choosing a degree — you’re procrastinating on making a real career decision.
2. Match Those Jobs to the Right Degree Family
Now connect those roles to the degree that actually feeds them:
- Mostly MPH territory
- Epidemiologist, surveillance officer, M&E specialist
- Public health program manager, health promotion officer
- Policy analyst in government, NGOs, or global-health agencies
- Mostly MHA territory
- Hospital administrator, health services manager
- Operations manager for specific service lines (ER, surgery, oncology, primary care)
- Quality improvement / patient safety manager
- Mostly MBA (with a health angle) territory
- Consultant in healthcare or general management
- Product / strategy / operations roles in healthtech, insurance, pharma, med-tech
- Corporate leadership tracks in big organizations (health or non-health)
If your list mixes “epidemiologist” and “management consultant” and “hospital CEO”, you’re not being “multi-passionate”. You’re undecided. Fix that first.
3. Decide How Much Career Flexibility You Actually Want
You can’t have maximum specialization and maximum flexibility at the same time. Pick your poison:
- You’re okay staying in public health / NGOs / government
- You like policy, programs, and population-level work.
- You’re comfortable living your whole career around ministries, UN agencies, big NGOs, and academic centers.
- An MPH makes sense.
- You’re okay staying inside hospitals and providers
- You want to run units, hospitals, or health systems.
- You like operations, staffing, budgets, and service delivery.
- An MHA is built for that track.
- You want the option to leave healthcare or jump sectors
- You might move into tech, finance, consulting, or startups later.
- You care a lot about brand, network, and cross-industry options.
- A serious MBA (with or without healthcare focus) gives you the broadest escape routes.
Be honest: if you know in your gut that you might leave health in 5–10 years, doing only a very narrow, health-only degree can box you in.
4. Look at Cost vs Realistic Payback, Not Fantasy Salaries
Stop reading “average salaries” and doing mental gymnastics.
For each concrete program on your list:
- Add up real total cost: tuition + living + exam fees + lost income.
- Check typical starting salaries in your country for realistic roles you can actually get (not the top LinkedIn flex job).
- Ask: “At that salary, how many years until I just get back to zero?”
Patterns you’ll usually see:
- MPH – often cheaper, strong for impact and stability, payback is fine if you hit UN/INGO/research roles, slower if you sink into the lowest-paid gov posts.
- MHA – mid–high cost, but hospital/health-system leadership can pay back reasonably fast if you don’t get stuck in the weakest employers.
- MBA – most expensive, biggest upside if you land in consulting/tech/strong corporate roles; a terrible deal if you pay premium tuition at a weak school with no serious recruiting.
If your spreadsheet only works when everything goes perfectly, you’re planning on luck, not on reality.
5. Country and School Brand Matter More Than You Want to Admit
Same letters, completely different outcomes depending on where and where from:
- An MPH from a country with strong public-health institutions and global-health presence gives you far more international options than a random local diploma.
- An MHA tied to big hospital systems or strong healthcare networks is a different beast from an unknown program nobody in the industry respects.
- An MBA with real pipelines into consulting/tech/healthcare leadership is worth considering. An MBA where recruiters don’t bother to visit is just expensive stationery.
The formula is not just MPH/MHA/MBA. It’s:
Degree type + Country + School brand + Network + Your actual skills
If you ignore that, you’ll end up angry at the letters instead of your decision process.
How These Degrees Play Out in Real Life (Example Profiles)
Now let’s stop being abstract. Here’s how MPH, MHA, and MBA usually look when you plug them into real people’s lives. If one of these profiles feels uncomfortably close to you, pay attention.
Profile 1 – Clinician Who Wants to Run Hospitals, Not Just Worked in Them
Background
- Doctor, nurse, dentist, pharmacist – already in the system.
- Enjoys fixing rotas, pathways, and processes more than doing a fifth identical clinic in a row.
- Long-term picture: medical director, COO, hospital CEO, or regional health-system leader.
Best move
- MHA first. That’s the direct route into operations, budgeting, workforce planning, and quality.
- Use it to step into roles like unit manager, department coordinator, or assistant administrator.
- Once you’re in serious leadership and want to jump into broader corporate/consulting roles, then consider an executive MBA or focused management programs.
What usually goes wrong
- Clinicians do an MPH, then get annoyed that they’re stuck writing reports, doing surveillance, or managing programs instead of running hospitals.
- Others jump straight into a vague MBA with no healthcare focus and wonder why hospital boards don’t treat them like experienced administrators.
If your dream involves bed occupancy, emergency flow, cost per case, and staff rosters, you’re describing an MHA world, not an MPH one.
Profile 2 – Public-Health-Facing Nurse or Field Worker Who Wants to Design Programs
Background
- Nurse, LHV, community health worker, social scientist, or NGO staff.
- Has seen villages, camps, or underserved urban areas up close.
- Motivated by prevention and equity, not by polishing hospital KPIs for private investors.
Best move
- A strong MPH with good field placements and real research work.
- Focus on epidemiology, health promotion, global health, or health policy & systems.
- Hunt for programs with real partnerships with ministries, NGOs, and UN agencies so your project work isn’t fake or purely academic.
What it leads to
- Designing and running community programs, district-level interventions, national campaigns, and evaluating what works.
- Roles in ministries, INGOs, UN projects, and research collaborations.
What usually breaks things
- Doing an MHA, then discovering you hate hospital politics, staff drama, and financial juggling.
- Doing a generic MBA and finding that corporate recruiters don’t value your health background, while public-health employers don’t care about your marketing class.
If the idea of field visits, surveys, focus groups, and M&E dashboards excites you more than management meetings, you’re clearly in MPH territory.
Profile 3 – Business / Tech Person Who Wants to Build or Scale Health Products
Background
- Comes from business, engineering, computer science, or data.
- Interested in digital health, AI in healthcare, wearable tech, insurance innovation, or med-tech.
- Wants roles like product manager, strategy lead, or consultant in health-related companies, not in ministries of health.
Best move
- A serious MBA with a clear healthtech or healthcare track.
- Look for programs where graduates actually end up at healthtech startups, insurers, pharma, big tech health divisions, or consulting firms.
- Stack your electives with digital health, healthcare strategy, and product/innovation courses.
What it leads to
- Building, launching, or scaling apps, platforms, or services used by patients, clinicians, or insurers.
- Sitting in meetings about roadmaps, user metrics, pricing, contracts, and partnerships, not vaccination microplans.
If you want to argue about user growth, churn, CAC, LTV, and product-market fit, not just prevalence and incidence, you need business training — that’s MBA language.
Profile 4 – Govt / NGO Health Officer Who Wants to Shape Policy, Not Just Execute It
Background
- Already in a department of health, program office, or NGO.
- Good sense of how the system works, but stuck at the “follow orders” level.
- Wants to move into epidemiology leadership, technical advisor roles, or policy design rather than hospital management.
Best move
- A rigorous MPH with depth in epidemiology and health policy & systems.
- Grab every chance for technical work: outbreak analysis, policy briefs, surveillance reports, publication-worthy research.
- Position yourself for roles like epidemiologist, technical officer, or policy advisor at national or international level.
What to add later
- Short management or leadership courses once you climb into senior roles. You don’t need a full MBA to chair a meeting or read a budget.
If you enjoy trend analysis, guidance documents, and program logic models more than org charts and profit lines, then MPH > MHA/MBA for you.
If none of these profiles comes close to how you see yourself, that’s the signal to stop shopping degrees and start doing some honest career exploration — conversations with people in the field, short internships, shadowing, and then coming back to this decision with clearer eyes.
How to Compare Specific Programs (MPH, MHA, or MBA) – Without Getting Scammed by Marketing
Once you’ve picked which type of degree fits your goals, the next mistake people make is thinking “any MPH/MHA/MBA will do.”
No. A weak program gives you debt, a PDF, and not much else.
Use this checklist to judge specific programs against each other.
1. Accreditation: Basic Sanity Check
If a program can’t clear the accreditation bar, that’s already a red flag.
- MPH
- Look for CEPH (or the main public-health accreditor in that country).
- Non-accredited programs can still be okay in some countries, but they need a strong reputation and real outcomes to compensate.
- MHA / Health Administration
- In some countries, CAHME or a similar body oversees health management degrees.
- If there is a well-known accreditor in your region and the program isn’t on the list, ask why.
- MBA
- Top business schools usually have at least one of AACSB, AMBA, or EQUIS.
- No accreditation doesn’t automatically mean “trash,” but combined with weak faculty and no recruiting, it’s a warning.
If the school avoids giving a straight answer on accreditation, walk away.
2. Curriculum: Does It Actually Match the Skills You Need?
Stop skimming course titles. Ask:
- Does the core give you the skills your target roles expect?
- MPH: solid epi, biostats, research methods, health policy/systems.
- MHA: healthcare finance, operations, quality, HR, health law/regulation.
- MBA: real finance, strategy, operations, analytics – not watered-down “executive hobby classes.”
- Are there electives that match where you want to go?
- Global health, implementation science, or advanced epi for MPH.
- Lean/Six Sigma, informatics, or service-line management for MHA.
- Digital health, healthtech, pharma, insurance, or entrepreneurship for MBA.
If the curriculum looks like a random buffet with no spine, it won’t build a coherent skill set.
3. Practicum / Residency / Internship: Is There Real Work or Just Busywork?
You learn more from one serious placement than from ten fluffy assignments.
Check:
- MPH
- Is there a real practicum with ministries, NGOs, UN agencies, or strong research groups?
- Do students work on genuine data, programs, and evaluations – or only hypothetical classroom projects?
- MHA
- Is there an administrative residency or fellowship embedded in a hospital or health system?
- Will you sit in actual management meetings and work on live operations/quality/finance problems?
- MBA
- Are internships and client projects part of the design?
- Which companies regularly host interns and projects – and do any of them match your target roles?
If students have to “arrange their own placements” with zero support, expect chaos and weak experience.
4. Outcomes: What Happens to Graduates in Reality?
Ignore the brochure hype. Look for hard evidence:
- Where do graduates actually work 12–24 months after finishing?
- What job titles do they hold?
- What countries or cities are they in?
- Do they end up in the sectors you care about (UN/NGOs, hospitals, consulting, healthtech, etc.)?
Steps:
- Stalk LinkedIn: search for “[Program Name] MPH/MHA/MBA” and see real profiles.
- Check if alumni landed roles similar to your target.
- See how long it took them to move into good positions after graduation.
If you can’t find alumni with decent jobs, that tells you more than any ranking.
5. Format: Online vs Hybrid vs On-Campus (Be Honest About Yourself)
- On-campus
- Best for building networks, access to faculty, and recruiting.
- More expensive and disruptive to your current life.
- Hybrid
- Some networking, some flexibility.
- Can work if you’re already in the field and just need the credential + structured learning.
- Online-only
- Flexible, sometimes cheaper.
- Networking is weaker; brand matters even more.
- You’ll only get value if you’re disciplined and already plugged into a professional environment.
If you know you struggle with self-discipline, don’t fool yourself with a pure online degree you’ll coast through and forget.
6. Cost, Funding, and Payback: Will This Degree Financially Punish You?
Don’t just look at the tuition number:
- Add tuition + fees + living costs + exam costs + lost income.
- Check scholarships, teaching assistantships, research assistantships, or employer funding.
- Then compare to realistic salaries for your target roles in your target country.
Ask:
“In a normal (not dream) job, how many years will it take to get back to zero?”
If that number scares you, either:
- Pick a different program,
- Change country,
- Or accept that your motivation is “I just want this degree emotionally,” and stop pretending it’s a rational financial move.
FAQs: MPH vs MHA vs MBA
Let’s kill the common questions directly.
Q: Is an MHA better than an MPH for healthcare management?
Short answer: Yes, for management inside hospitals and health systems, an MHA is usually more relevant.
- MHA = built around operations, finance, HR, quality, and regulation in provider organizations.
- MPH = built around populations, programs, and policy, not daily hospital logistics.
If you want to manage wards, clinics, or hospitals, MPH alone is the wrong tool.
Q: Is an MBA better than an MHA for healthcare leadership?
It depends where you want to lead.
- If you want to be a senior leader inside hospitals or provider systems, an MHA (especially from a respected school) is very strong.
- If you want healthcare leadership in corporate settings (healthtech, insurance, pharma, consulting), a health-focused MBA usually has more weight.
Blunt version:
- Hospital CEO track → MHA (optionally plus MBA later).
- Corporate/consulting/healthtech leadership → MBA.
Q: Does an MPH usually pay less than an MHA or MBA?
In most markets: yes.
- MPH roles are often in government, NGOs, and academia – stable, meaningful, but not the best-paid.
- MHA/MBA roles tend to be in management and corporate tracks, which usually pay more, especially at senior levels.
There are exceptions (UN, big INGOs, elite research centers), but the basic pattern holds: management and corporate roles generally have higher income ceilings than pure public-health roles.
Q: Can I work outside healthcare with an MHA?
Technically yes, practically limited.
- Your training and experience are tuned to healthcare delivery systems.
- You might move into related industries (insurance, healthtech, some consulting), but jumping to totally unrelated sectors is harder.
If you want broad cross-industry options, MBA beats MHA.
If you’re happy to stay near health, MHA is fine.
Q: Is an MPH good for becoming a hospital administrator?
Not by itself.
- An MPH can help with quality, infection control, community outreach, or population-health strategy, but it doesn’t train you in daily operations, staffing, and hospital finance.
- Some people do MPH + on-the-job experience and still end up in admin roles, but they’re swimming upstream.
If your main dream is hospital administration, do MHA or at least MHA-style training, not just an MPH.
Q: Can I combine degrees (MD/MPH, MBA/MPH, MHA/MBA, etc.)? Is that smart?
You can; the question is whether you need to.
- MD/MPH – useful if you want to move into public health, policy, global health, or research while keeping clinical credibility.
- MBA/MPH – strong if you want to mix public health + business (healthtech, social enterprises, health-focused consulting).
- MHA/MBA – sometimes valuable if you’re already in leadership and want to jump from hospital systems into broader corporate or consulting roles.
But:
- Doing multiple degrees because you’re lost is a bad strategy.
- One well-chosen degree + relevant experience usually beats 3 random diplomas with no clear direction.
Q: Which degree is best if I want to work in global health?
Most of the time: MPH.
- Global health jobs care about epi, health systems, policy, implementation, and M&E.
- An MPH from a program with strong global-health links plus field experience beats an MBA/MHA with no global-health focus.
An MBA or MHA only makes sense here if you’re targeting management or strategy roles inside big global-health organizations or healthtech companies, not frontline program or policy work.
Q: Which degree is best if I want to work in consulting?
- If you want big-name consulting firms (especially strategy firms): MBA from a school they actually recruit at.
- For niche health-policy or health-systems consulting, an MPH from a strong institution can work, but the path is narrower and more technical.
- MHA can get you into operations-focused healthcare consulting, especially around hospitals and providers, but won’t be as broad as an MBA.
If “consulting” is your word for “I don’t know what I want, but I want status and high pay,” fix that first.
Q: Do employers care more about the school name or the specific degree?
Both matter, but brand + outcomes usually beat the exact letters.
- A well-known school with strong alumni and employer ties can push a “lower” degree further.
- A no-name institution offering the “perfect” degree on paper can still leave you stuck.
Rough hierarchy:
School brand + network + your experience > exact acronym on the diploma.
That doesn’t mean the degree type is irrelevant; it means that picking MPH vs MHA vs MBA is step one. Picking a good program and then actually doing something useful with it is what really moves your career.
Internal Links:
CEPH-Accredited MPH Programs in New York (2025)
Accelerated 1-Year MPH Programs (2025 Guide): Accredited 12-Month MPH Options
Related MPH Guides
Use these linked guides to compare degree fit, accreditation, and costs before you apply.
